

The association between age and the development of respiratory syncytial virus neutralising antibody responses following natural infection in infants
- PMID: 25005882
- PMCID: PMC4141889
- DOI: 10.1016/j.vaccine.2014.05.038
The association between age and the development of respiratory syncytial virus neutralising antibody responses following natural infection in infants
Abstract
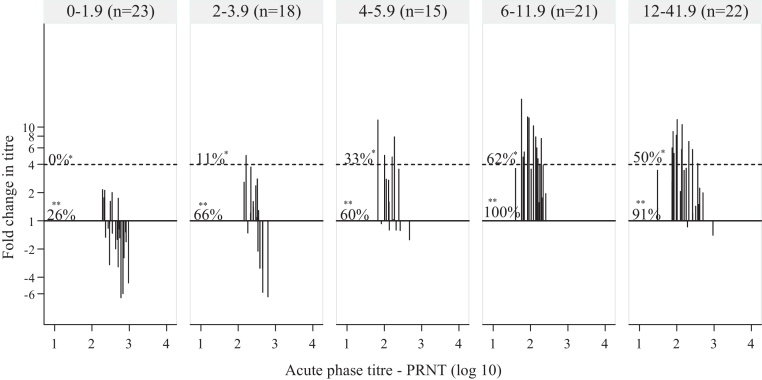
To determine the age at which infants mount significant neutralising antibody responses to both natural RSV infection and live vaccines that mimic natural infection, RSV-specific neutralising antibodies in the acute and convalescent phase sera of infants with RSV infection were assayed. Age-specific incidence estimates for hospitalisation with severe RSV disease were determined and compared to age-specific neutralising antibody response patterns. Disease incidence peaked at between 2 and 3.9 months of life. Following natural infection, relative to the mean acute phase antibody titre, the mean convalescent titre was lower in the 0-1.9 month age class, no different in the 2-3.9 month age class and greater in all age classes greater than 4 months. These data suggest effective vaccination with live vaccines that mimic natural infection may not be achieved before the age of 4 months. Maternal vaccination may be an alternative to direct infant vaccination in order to protect very young babies.
Keywords: Immunity; Neutralising antibody; Respiratory syncytial virus.
Copyright © 2014 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures

References
-
- Falsey A.R., Hennessey P.A., Formica M.A., Cox C., Walsh E.E. Respiratory syncytial virus infection in elderly and high-risk adults. N Engl J Med. 2005;352:1749–1759. - PubMed
-
- Johnson J.E., Gonzales R.A., Olson S.J., Wright P.F., Graham B.S. The histopathology of fatal untreated human respiratory syncytial virus infection. Mod Pathol. 2007;20:108–119. - PubMed
-
- Blanken M.O., Rovers M.M., Molenaar J.M., Winkler-Seinstra P.L., Meijer A., Kimpen J.L. Respiratory syncytial virus and recurrent wheeze in healthy preterm infants. N Engl J Med. 2013;368:1791–1799. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
