

Clinical characterization and survival of patients with borderline elevation in pulmonary artery pressure
- PMID: 25006408
- PMCID: PMC4070822
- DOI: 10.1086/674756
Clinical characterization and survival of patients with borderline elevation in pulmonary artery pressure
Abstract
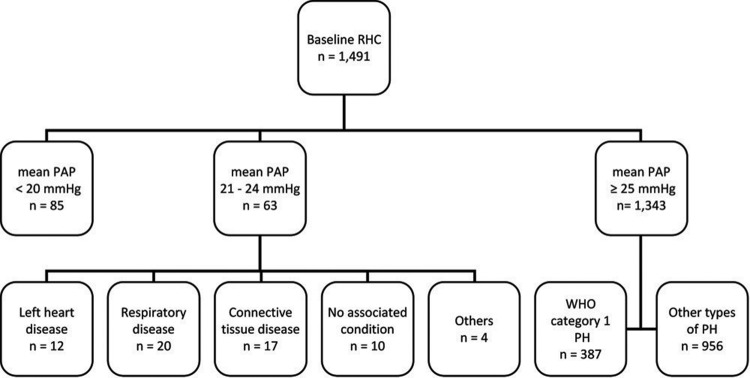
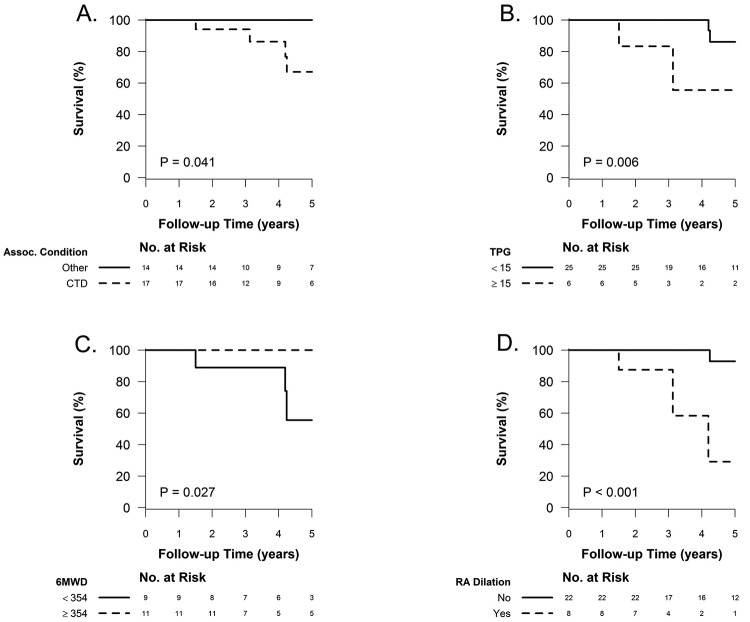
Normal resting mean pulmonary artery pressure (PAP) is 8-20 mmHg. Pulmonary hypertension is defined as mean PAP of ≥25 mmHg. Borderline PAP levels of 21-24 mmHg are of unclear significance. We sought to determine the clinical characteristics and survival of subjects with mean PAP of 21-24 mmHg. We examined 1,491 patients enrolled in the Cleveland Clinic Pulmonary Hypertension Registry between February 1990 and May 2012 with baseline right heart catheterization. The relationship between PAP and all-cause mortality was assessed by Cox models and a tree-based analysis. Sixty-three patients had borderline PAP (underlying conditions: 12 left heart disease, 20 respiratory disease, 17 connective-tissue disease, 4 others, and 10 none). We then compared 3 groups: borderline PAP without heart or lung disease ([Formula: see text]), normal PAP without heart or lung disease ([Formula: see text]), and category 1 pulmonary arterial hypertension (PAH; [Formula: see text]). Borderline-PAP patients had levels of hemodynamic and functional compromise between those for normal-PAP patients and those for patients with PAH. Borderline PAP was associated with increased mortality compared to normal PAP (hazard ratio: 4.03 [95% confidence interval: 0.78-20.80], [Formula: see text]). A tree-based analysis demonstrated almost identical cut points in mean PAP (≤20, 21-26, and ≥27 mmHg) associated with differential survival ([Formula: see text]). Connective-tissue disease and an elevated transpulmonary gradient were predictors of worse survival in the borderline-PAP population. Borderline PAP elevation is associated with decreased survival, particularly in the context of connective-tissue disease and an elevated transpulmonary gradient.
Keywords: pulmonary artery pressure; pulmonary heart disease; pulmonary hypertension; survival.
Figures
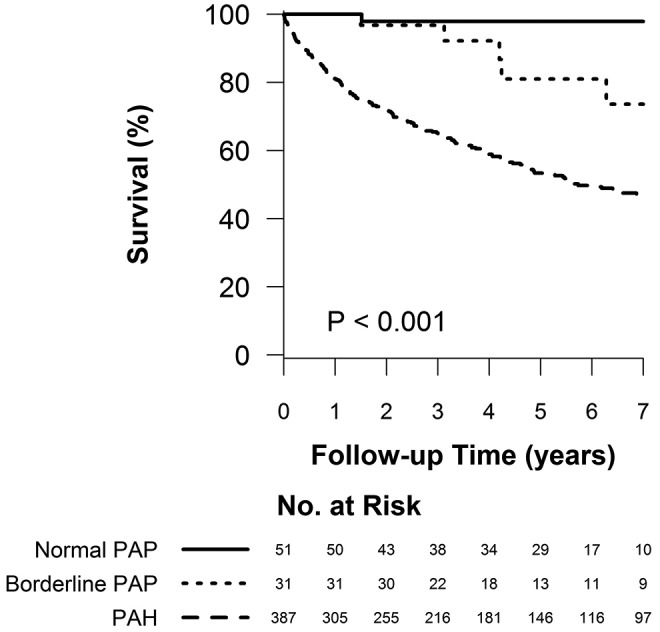
 for the pairwise comparison between normal and borderline PAP;
for the pairwise comparison between normal and borderline PAP;  for the pairwise comparison between group 1 PAH and borderline PAP.
for the pairwise comparison between group 1 PAH and borderline PAP.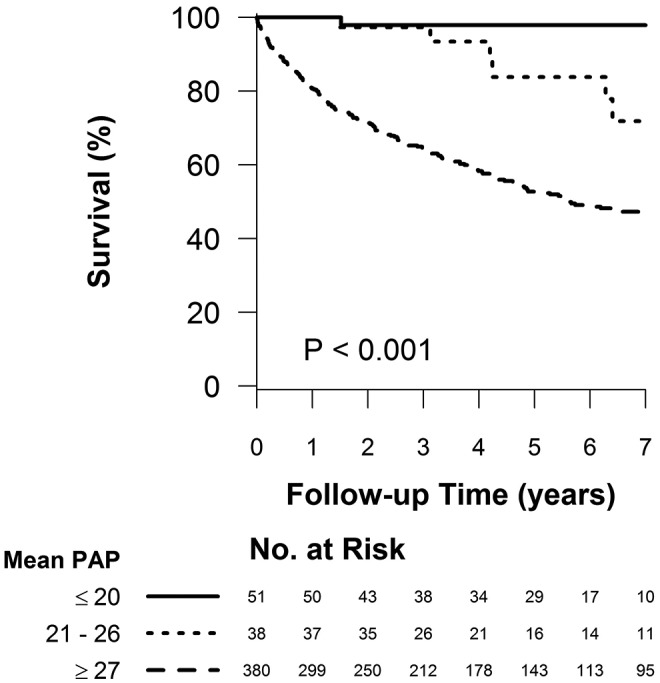
 for the pairwise comparison between mean pulmonary artery pressures (PAPs) of ≤20 and 21–26 mmHg;
for the pairwise comparison between mean pulmonary artery pressures (PAPs) of ≤20 and 21–26 mmHg;  for the pairwise comparison between mean PAPs of 21–26 and ≥27 mmHg.
for the pairwise comparison between mean PAPs of 21–26 and ≥27 mmHg.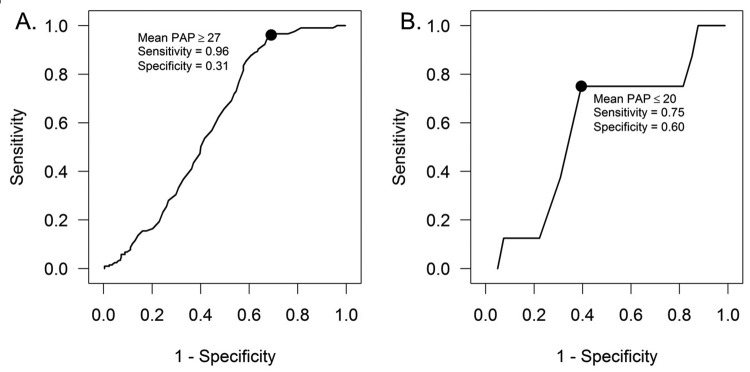
References
-
- Batal O, Khatib OF, Bair N, Aboussouan LS, Minai OA. Sleep quality, depression, and quality of life in patients with pulmonary hypertension. Lung 2011;189(2):141–149. - PubMed
-
- Copher R, Cerulli A, Watkins A, Monsalvo ML. Treatment patterns and healthcare system burden of managed care patients with suspected pulmonary arterial hypertension in the United States. J Med Econ 2012;15(5):947–955. - PubMed
-
- D’Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, Fishman AP, et al. Survival in patients with primary pulmonary hypertension: results from a national prospective registry. Ann Intern Med 1991;115(5):343–349. - PubMed
-
- Humbert M, Sitbon O, Chaouat A, Bertocchi M, Habib G, Gressin V, Yaïci A, et al. Survival in patients with idiopathic, familial, and anorexigen-associated pulmonary arterial hypertension in the modern management era. Circulation 2010;122(2):156–163. - PubMed
-
- Galiè N, Palazzini M, Manes A. Pulmonary hypertension and pulmonary arterial hypertension: a clarification is needed. Eur Respir J 2010;36(5):986–990. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
