

State of the art: advanced imaging of the right ventricle and pulmonary circulation in humans (2013 Grover Conference series)
- PMID: 25006434
- PMCID: PMC4070773
- DOI: 10.1086/675978
State of the art: advanced imaging of the right ventricle and pulmonary circulation in humans (2013 Grover Conference series)
Abstract
Pulmonary arterial hypertension (PAH) is a progressive disease characterized by remodeling and vasoconstriction of the pulmonary vasculature, ultimately leading to right ventricular (RV) failure and death. Recent developments in echocardiography, cardiovascular magnetic resonance imaging, computed tomography, and positron emission tomography allow advanced, noninvasive, in vivo assessment of the RV and have contributed to the identification of risk factors, prognostic factors, and monitoring of therapeutic responses in patients with PAH. Although far from reaching its future potential, these techniques have not only provided global RV assessment but also allowed evaluation of changes in cellular and molecular tissue processes, such as metabolism, oxygen balance and ischemia, angiogenesis, and apoptosis. Integrated application of these techniques could provide full insights into the different pathophysiological aspects of a failing RV in the setting of PAH. Recent advances in hybrid imaging have implemented simultaneous measurements of myocardial and vascular interactions and will be one of the most important potential future developments.
Keywords: cardiovascular magnetic resonance imaging; echocardiography; positron emission tomography; pulmonary arterial hypertension; right ventricle.
Figures
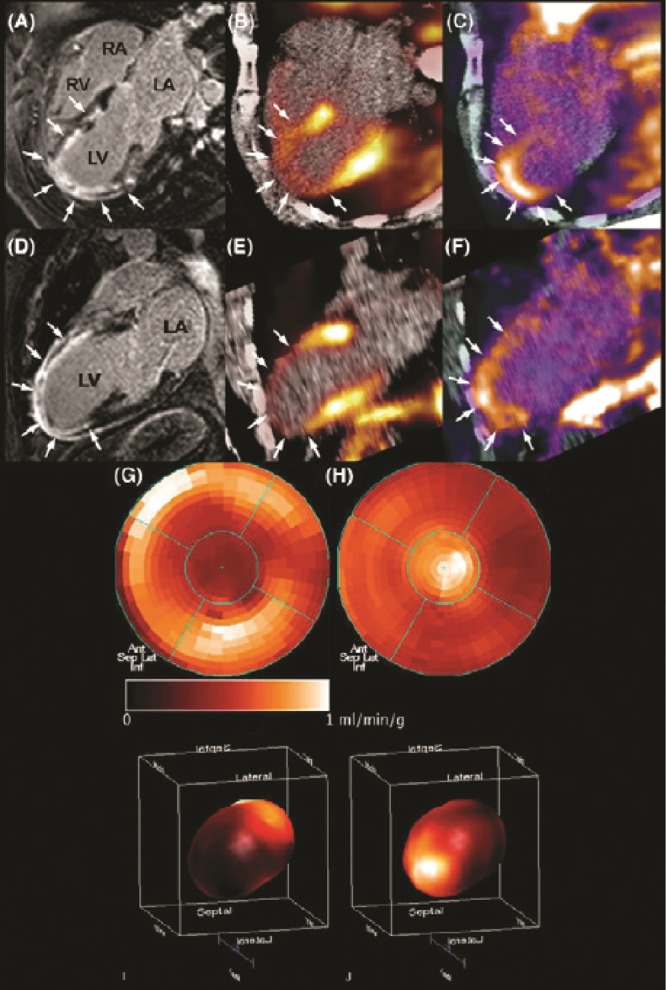
 integrins, demonstrated focal signal areas in the infarcted area (C, F). This signal may reflect angiogenesis within the healing area (arrows). Polar maps of myocardial blood flow assessed by PET with 13N-ammonia (G, I) show severely reduced blood flow in the distal left anterior descending coronary artery perfusion region. Co-localized 18F-RGD signal corresponded to the regions of reduced blood flow (H, J), demonstrating the extent of the
integrins, demonstrated focal signal areas in the infarcted area (C, F). This signal may reflect angiogenesis within the healing area (arrows). Polar maps of myocardial blood flow assessed by PET with 13N-ammonia (G, I) show severely reduced blood flow in the distal left anterior descending coronary artery perfusion region. Co-localized 18F-RGD signal corresponded to the regions of reduced blood flow (H, J), demonstrating the extent of the  integrin expression in the infarcted area. Reprinted with permission from Makowski et al.
integrin expression in the infarcted area. Reprinted with permission from Makowski et al.Similar articles
-
The right ventricle under pressure: evaluating the adaptive and maladaptive changes in the right ventricle in pulmonary arterial hypertension using echocardiography (2013 Grover Conference series).Pulm Circ. 2015 Mar;5(1):29-47. doi: 10.1086/679699. Pulm Circ. 2015. PMID: 25992269 Free PMC article. Review.
-
Cardiac magnetic resonance imaging: what can it add to our knowledge of the right ventricle in pulmonary arterial hypertension?Am J Cardiol. 2012 Sep 15;110(6 Suppl):25S-31S. doi: 10.1016/j.amjcard.2012.06.013. Am J Cardiol. 2012. PMID: 22921028 Review.
-
The right ventricle in scleroderma (2013 Grover Conference Series).Pulm Circ. 2015 Mar;5(1):3-14. doi: 10.1086/679607. Pulm Circ. 2015. PMID: 25992267 Free PMC article. Review.
-
Noninvasive assessment of right ventricular function: will there be resurgence in radionuclide imaging techniques?Curr Cardiol Rep. 2010 Mar;12(2):162-9. doi: 10.1007/s11886-010-0092-y. Curr Cardiol Rep. 2010. PMID: 20425172 Review.
-
The adrenergic system in pulmonary arterial hypertension: bench to bedside (2013 Grover Conference series).Pulm Circ. 2015 Sep;5(3):415-23. doi: 10.1086/682223. Pulm Circ. 2015. PMID: 26401244 Free PMC article. Review.
Cited by
-
Dietary intake and glutamine-serine metabolism control pathologic vascular stiffness.Cell Metab. 2024 Jun 4;36(6):1335-1350.e8. doi: 10.1016/j.cmet.2024.04.010. Epub 2024 May 2. Cell Metab. 2024. PMID: 38701775 Free PMC article.
-
Non-invasive Multimodality Cardiovascular Imaging of the Right Heart and Pulmonary Circulation in Pulmonary Hypertension.Front Cardiovasc Med. 2019 Mar 14;6:24. doi: 10.3389/fcvm.2019.00024. eCollection 2019. Front Cardiovasc Med. 2019. PMID: 30931315 Free PMC article. Review.
-
Relationship of Right Ventricular Size and Function with Respiratory Status in Duchenne Muscular Dystrophy.Pediatr Cardiol. 2016 Jun;37(5):878-83. doi: 10.1007/s00246-016-1362-2. Epub 2016 Mar 2. Pediatr Cardiol. 2016. PMID: 26936620
-
Characterization of pulmonary arterial stiffness using cardiac MRI.Int J Cardiovasc Imaging. 2024 Feb;40(2):425-439. doi: 10.1007/s10554-023-02989-6. Epub 2023 Oct 30. Int J Cardiovasc Imaging. 2024. PMID: 37902921 Review.
-
Pulmonary Hypertension in Intensive Care Units: An Updated Review.Tanaffos. 2019 Mar;18(3):180-207. Tanaffos. 2019. PMID: 32411259 Free PMC article. Review.
References
-
- Starr I, Jeffers WA, Meade RH. The absence of conspicuous increments of venous pressure after severe damage to the RV of the dog, with discussion of the relation between clinical congestive heart failure and heart disease. Am Heart J 1943;26:291–301.
-
- Haddad F, Doyle R, Murphy DJ, Hunt SA. Right ventricular function in cardiovascular disease, part II: pathophysiology, clinical importance, and management of right ventricular failure. Circulation 2008;117(13):1717–1731. - PubMed
-
- McLaughlin VV, McGoon MD. Pulmonary arterial hypertension. Circulation 2006;114(13):1417–1431. - PubMed
-
- Voelkel NF, Quaife RA, Leinwand LA, Barst RJ, McGoon MD, Meldrum DR, et al. Right ventricular function and failure: report of a National Heart, Lung, and Blood Institute working group on cellular and molecular mechanisms of right heart failure. Circulation 2006;114(17):1883–1891. - PubMed
-
- Stevens GR, Garcia-Alvarez A, Sahni S, Garcia MJ, Fuster V, Sanz J. RV dysfunction in pulmonary hypertension is independently related to pulmonary artery stiffness. JACC Cardiovasc Imaging 2012;5(4):378–387. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
