

Screening for germline mismatch repair mutations following diagnosis of sebaceous neoplasm
- PMID: 25006859
- PMCID: PMC4977578
- DOI: 10.1001/jamadermatol.2014.1217
Screening for germline mismatch repair mutations following diagnosis of sebaceous neoplasm
Abstract
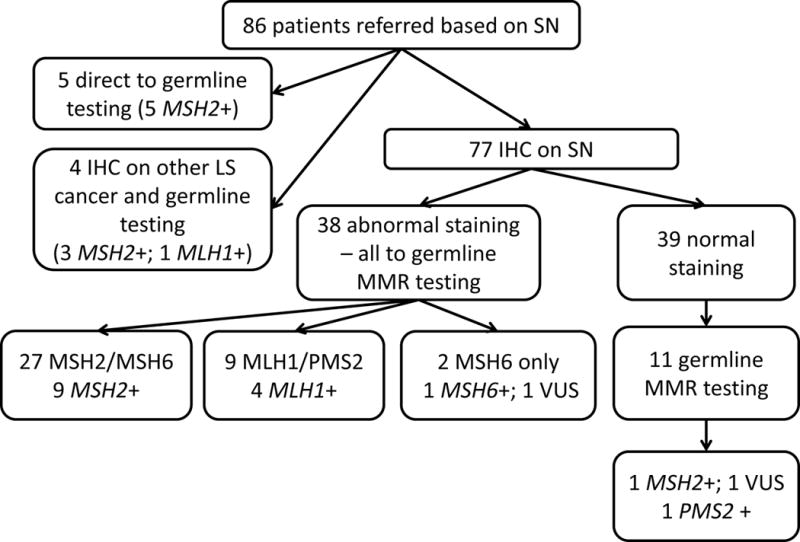
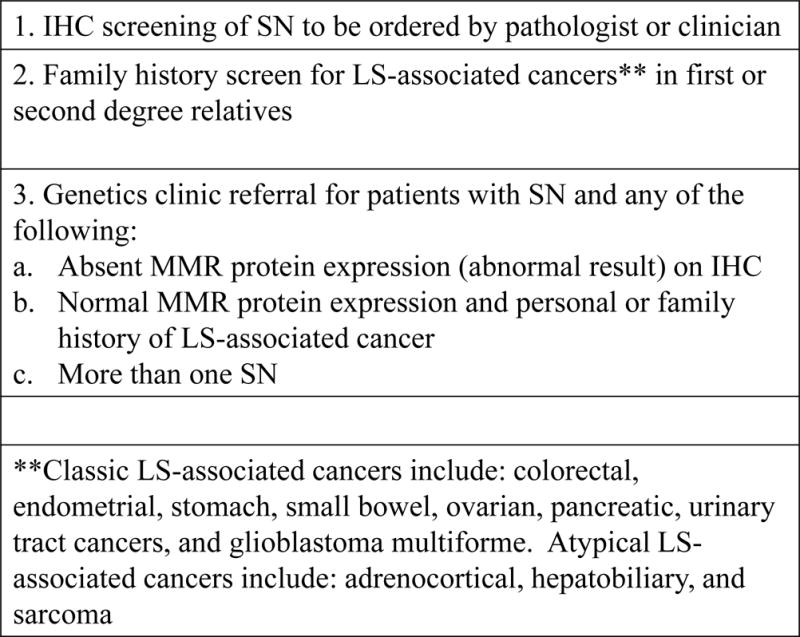
IMPORTANCE Sebaceous neoplasms (SNs) define the Muir-Torre syndrome variant of Lynch syndrome (LS), which is associated with increased risk for colon and other cancers necessitating earlier and more frequent screening to reduce morbidity and mortality.Immunohistochemical (IHC) staining for mismatch repair (MMR) proteins in SNs can be used to screen for LS, but data on subsequent germline genetic testing to confirm LS diagnosis are limited.OBJECTIVE To characterize the utility of IHC screening of SNs in identification of germline MMR mutations confirming LS.DESIGN, SETTING, AND PARTICIPANTS Retrospective study at 2 academic cancer centers of 86 adult patients referred for clinical genetics evaluation after diagnosis of SN.MAIN OUTCOMES AND MEASURES Results of tumor IHC testing and germline genetic testing were reviewed to determine positive predictive value and sensitivity of IHC testing in diagnosis of LS. Clinical variables, including age at diagnosis of SN, clinical diagnostic criteria for LS and Muir-Torre syndrome, and family history characteristics were compared between mutation carriers and noncarriers.RESULTS Of 86 patients with SNs, 25 (29%) had germline MMR mutations confirming LS.Among 77 patients with IHC testing on SNs, 38 (49%) had loss of staining of 1 or more MMR proteins and 14 had germline MMR mutations. Immunohistochemical analysis correctly identified 13 of 16 MMR mutation carriers, corresponding to 81% sensitivity. Ten of 12 patients(83%) with more than 1 SN had MMR mutations. Fifty-two percent of MMR mutation carriers did not meet clinical diagnostic criteria for LS, and 11 of 25 (44%) did not meet the clinical definition of Muir-Torre syndrome. CONCLUSIONS AND RELEVANCE Immunohistochemical screening of SNs is effective in identifying patients with germline MMR mutations and can be used as a first-line test when LSis suspected. Abnormal IHC results, including absence of MSH2, are not diagnostic of LS and should be interpreted cautiously in conjunction with family history and germline genetic testing. Use of family history to select patients for IHC screening has substantial limitations,suggesting that universal IHC screening of SNs merits further study. Clinical genetics evaluation is warranted for patients with abnormal IHC test results, normal IHC test results with personal or family history of other LS-associated neoplasms, and/or multiple SNs.
Conflict of interest statement
Financial Conflict of Interest Disclosure: None reported
All Financial Interests: Dr. Gruber, Ms. Everett, and Ms. Gustafson have served as paid consultants to Myriad Genetic Laboratories, Inc.
Figures
Similar articles
-
Importance of universal mismatch repair protein immunohistochemistry in patients with sebaceous neoplasia as an initial screening tool for Muir-Torre syndrome.Hum Pathol. 2016 Mar;49:1-9. doi: 10.1016/j.humpath.2015.10.005. Epub 2015 Oct 31. Hum Pathol. 2016. PMID: 26826402
-
An Intrapatient Concordance Study of Mismatch Repair Protein Immunohistochemical Staining Patterns in Patients With Muir-Torre Syndrome.JAMA Dermatol. 2020 Jun 1;156(6):676-680. doi: 10.1001/jamadermatol.2020.0433. JAMA Dermatol. 2020. PMID: 32267475 Free PMC article.
-
Tumor mismatch repair immunohistochemistry and DNA MLH1 methylation testing of patients with endometrial cancer diagnosed at age younger than 60 years optimizes triage for population-level germline mismatch repair gene mutation testing.J Clin Oncol. 2014 Jan 10;32(2):90-100. doi: 10.1200/JCO.2013.51.2129. Epub 2013 Dec 9. J Clin Oncol. 2014. PMID: 24323032 Free PMC article.
-
Muir-Torre Syndrome and founder mismatch repair gene mutations: A long gone historical genetic challenge.Gene. 2016 Sep 10;589(2):127-32. doi: 10.1016/j.gene.2015.06.078. Epub 2015 Jul 2. Gene. 2016. PMID: 26143115 Review.
-
Mismatch repair genes founder mutations and cancer susceptibility in Lynch syndrome.Clin Genet. 2015 Jun;87(6):507-16. doi: 10.1111/cge.12529. Epub 2014 Dec 9. Clin Genet. 2015. PMID: 25345868 Review.
Cited by
-
Sebaceous carcinoma: an updated review of pathogenesis, diagnosis, and treatment options.Arch Dermatol Res. 2023 Dec 19;316(1):55. doi: 10.1007/s00403-023-02747-7. Arch Dermatol Res. 2023. PMID: 38112896 Review.
-
Pharmacogenetic Review: Germline Genetic Variants Possessing Increased Cancer Risk With Clinically Actionable Therapeutic Relationships.Front Genet. 2022 May 24;13:857120. doi: 10.3389/fgene.2022.857120. eCollection 2022. Front Genet. 2022. PMID: 35685436 Free PMC article. Review.
-
A retrospective cohort study of genetic referral and diagnosis of Lynch syndrome in patients with cutaneous sebaceous lesions.Fam Cancer. 2023 Jul;22(3):295-301. doi: 10.1007/s10689-022-00322-z. Epub 2022 Nov 28. Fam Cancer. 2023. PMID: 36437392
-
Looking beyond the surface: Muir Torre syndrome.Arch Clin Cases. 2023 Sep 20;10(3):119-122. doi: 10.22551/2023.40.1003.10255. eCollection 2023. Arch Clin Cases. 2023. PMID: 37736596 Free PMC article.
-
Germline Testing of Mismatch Repair Genes Is Needed in the Initial Evaluation of Patients With Muir-Torre Syndrome-Associated Cutaneous Sebaceous Neoplasms: A Case Series.Cureus. 2023 Jan 19;15(1):e33975. doi: 10.7759/cureus.33975. eCollection 2023 Jan. Cureus. 2023. PMID: 36824550 Free PMC article.
References
-
- The Proceedings of the Collaborative Group of the Americas on Inherited Colorectal Cancer Sheraton Boston Hotel, Boston, Massachusetts, October 27–29, 2012. Fam Cancer. 2013 doi: 10.1007/s10689-012-9592-9. Epub 2013/05/03. - DOI
-
- Torre D. Multiple sebaceous tumors. Arch Dermatol. 1968;98(5):549–51. Epub 1968/11/01. - PubMed
-
- Lynch HT, Lynch PM, Pester J, Fusaro RM. The cancer family syndrome. Rare cutaneous phenotypic linkage of Torre’s syndrome. Arch Intern Med. 1981;141(5):607–11. Epub 1981/04/01. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
