

Subtyping attention-deficit/hyperactivity disorder using temperament dimensions: toward biologically based nosologic criteria
- PMID: 25006969
- PMCID: PMC4278404
- DOI: 10.1001/jamapsychiatry.2014.763
Subtyping attention-deficit/hyperactivity disorder using temperament dimensions: toward biologically based nosologic criteria
Retracted and republished in
-
Notice of Retraction and Replacement. Karalunas et al. Subtyping attention-deficit/hyperactivity disorder using temperament dimensions: toward biologically based nosologic criteria. JAMA Psychiatry. 2014;71(9):1015-1024.JAMA Psychiatry. 2018 Apr 1;75(4):408-409. doi: 10.1001/jamapsychiatry.2018.0013. JAMA Psychiatry. 2018. PMID: 29516086 Free PMC article. No abstract available.
Abstract
Importance: Psychiatric nosology is limited by behavioral and biological heterogeneity within existing disorder categories. The imprecise nature of current nosologic distinctions limits both mechanistic understanding and clinical prediction. We demonstrate an approach consistent with the National Institute of Mental Health Research Domain Criteria initiative to identify superior, neurobiologically valid subgroups with better predictive capacity than existing psychiatric categories for childhood attention-deficit/hyperactivity disorder (ADHD).
Objective: To refine subtyping of childhood ADHD by using biologically based behavioral dimensions (i.e., temperament), novel classification algorithms, and multiple external validators.
Design, setting, and participants: A total of 437 clinically well-characterized, community-recruited children, with and without ADHD, participated in an ongoing longitudinal study. Baseline data were used to classify children into subgroups based on temperament dimensions and examine external validators including physiological and magnetic resonance imaging measures. One-year longitudinal follow-up data are reported for a subgroup of the ADHD sample to address stability and clinical prediction.
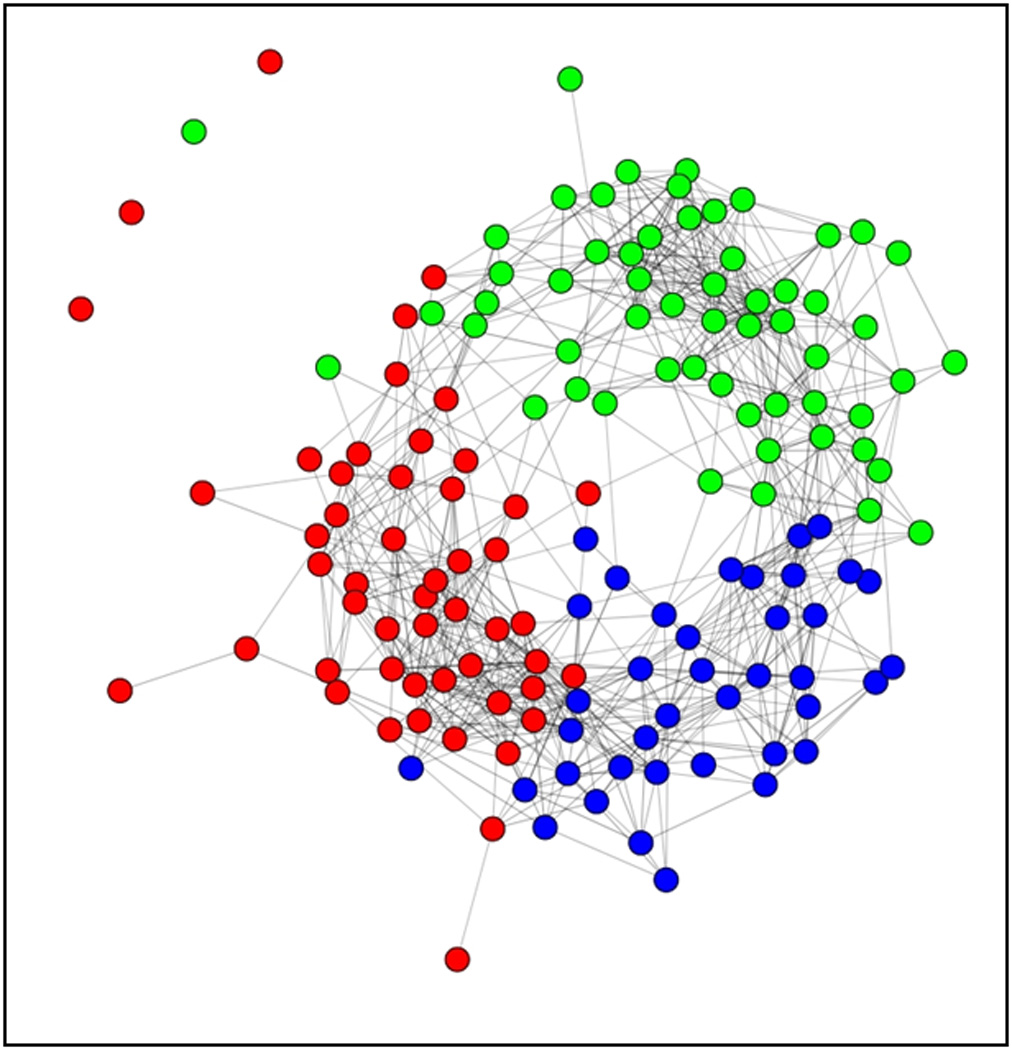
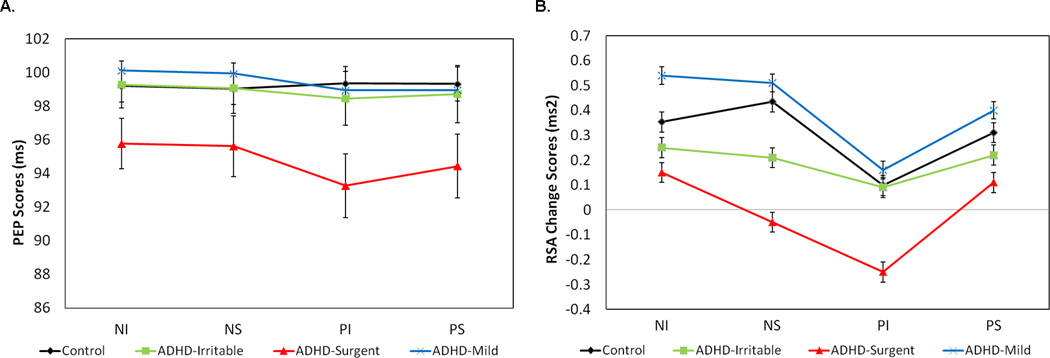
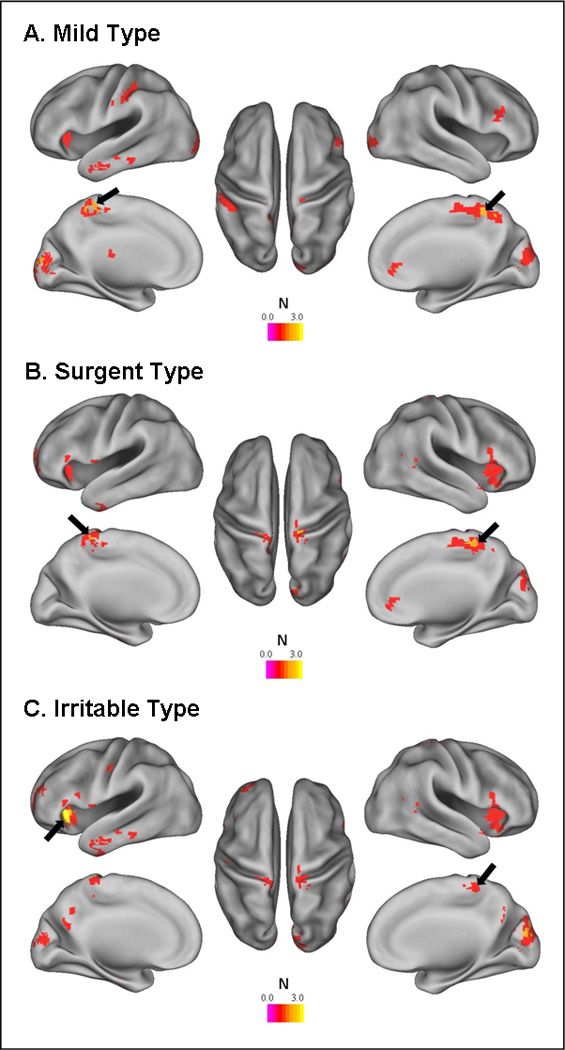
Main outcomes and measures: Parent/guardian ratings of children on a measure of temperament were used as input features in novel community detection analyses to identify subgroups within the sample. Groups were validated using 3 widely accepted external validators: peripheral physiological characteristics (cardiac measures of respiratory sinus arrhythmia and pre-ejection period), central nervous system functioning (via resting-state functional connectivity magnetic resonance imaging), and clinical outcomes (at 1-year longitudinal follow-up).
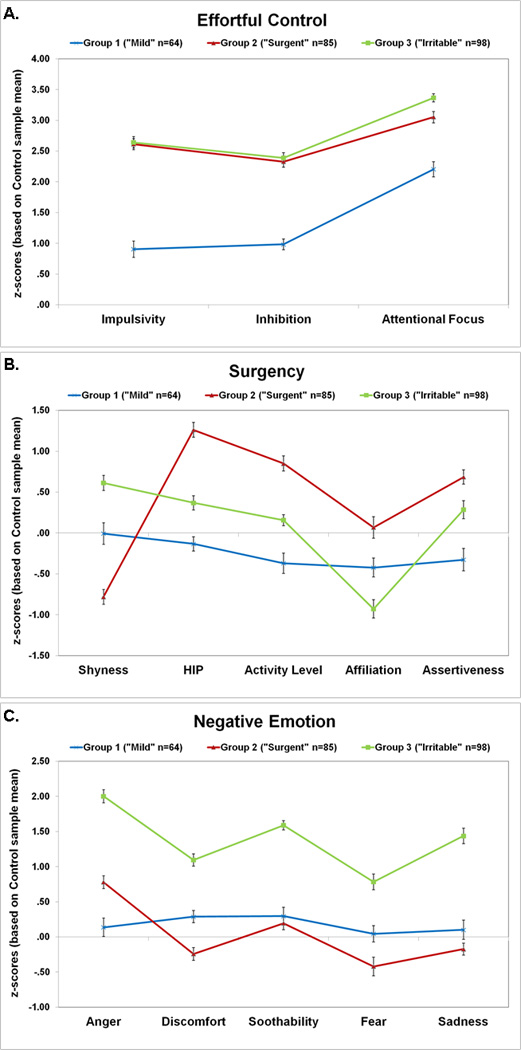
Results: The community detection algorithm suggested 3 novel types of ADHD, labeled as mild (normative emotion regulation), surgent (extreme levels of positive approach-motivation), and irritable (extreme levels of negative emotionality, anger, and poor soothability). Types were independent of existing clinical demarcations including DSM-5 presentations or symptom severity. These types showed stability over time and were distinguished by unique patterns of cardiac physiological response, resting-state functional brain connectivity, and clinical outcomes 1 year later.
Conclusions and relevance: Results suggest that a biologically informed temperament-based typology, developed with a discovery-based community detection algorithm, provides a superior description of heterogeneity in the ADHD population than does any current clinical nosologic criteria. This demonstration sets the stage for more aggressive attempts at a tractable, biologically based nosology.
Conflict of interest statement
Figures
References
-
- Doyle AE, et al. Are endophenotypes based on measures of executive functions useful for molecular genetic studies of ADHD? Journal of Child Psychology and Psychiatry. 2005;46(7):778–803. - PubMed
-
- Insel T, et al. Research domain criteria (RDoC): Toward a new classification framework for research on mental disorders. The American Journal of Psychiatry. 2010;167(7):748–751. - PubMed
-
- Faraone SV. Genetics of childhood disorders: XX. ADHD, part 4: Is ADHD genetically heterogeneous? Journal of the American Academy of Child & Adolescent Psychiatry. 2000;39(11):1455–1457. - PubMed
-
- Todd RD. Genetics of childhood disorders: XXI. ADHD, Part 5: A behavioral genetic perspective. Journal of the American Academy of Child & Adolescent Psychiatry. 2000;39(12):1571–1573. - PubMed
-
- Khan SA, Faraone SV. The genetics of ADHD: a literature review of 2005. Current Psychiatry Reports. 2006;8(5):393. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
