

Efficacy and safety of fluticasone furoate 100 μg and 200 μg once daily in the treatment of moderate-severe asthma in adults and adolescents: a 24-week randomised study
- PMID: 25007865
- PMCID: PMC4107726
- DOI: 10.1186/1471-2466-14-113
Efficacy and safety of fluticasone furoate 100 μg and 200 μg once daily in the treatment of moderate-severe asthma in adults and adolescents: a 24-week randomised study
Abstract
Background: Inhaled corticosteroids are a mainstay of therapy for persistent asthma, but suboptimal adherence with twice-daily use is widespread. Fluticasone furoate (FF) is a new inhaled corticosteroid (ICS) suitable for once-daily dosing in asthma. This study was performed to descriptively assess the efficacy and safety of two doses of FF, with no planned formal statistical hypothesis testing.
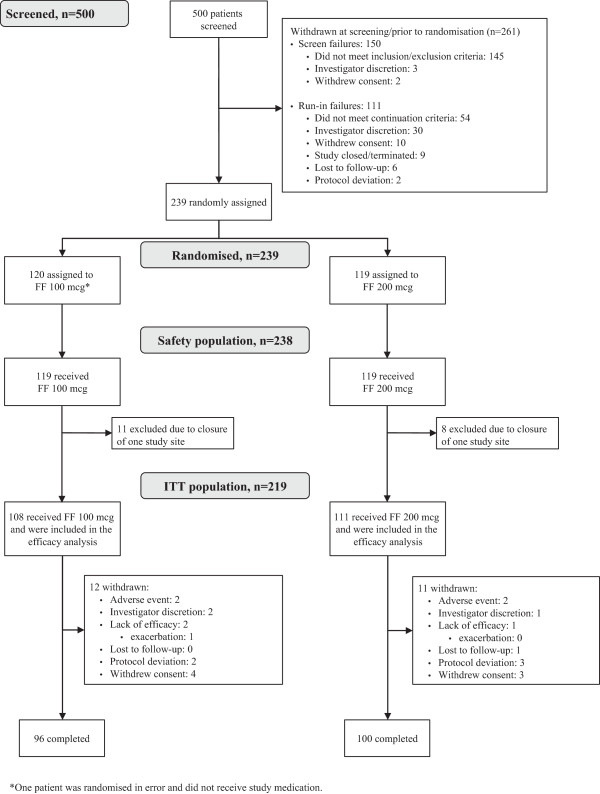
Methods: This was a 24-week double-blind, multicentre, parallel-group study (NCT01431950). Patients aged ≥ 12 years with moderate-severe persistent asthma and uncontrolled on mid-high dose ICS were stratified by baseline FEV1 and randomised (1:1) to treatment with FF 100 μg or 200 μg once daily in the evening. The primary endpoint was change from baseline trough FEV1 after 24 weeks; secondary and other endpoints included peak expiratory flow (PEF) and rescue-free and symptom-free 24-hour periods over Weeks 1-24, and Asthma Control Test™ (ACT) score at Week 24. A pre-specified subgroup analysis of patients by randomisation strata was performed for the primary and selected secondary and other endpoints. Safety assessments included adverse events, laboratory and vital sign measurements, and change from baseline in 24-hour urinary cortisol at Week 24.
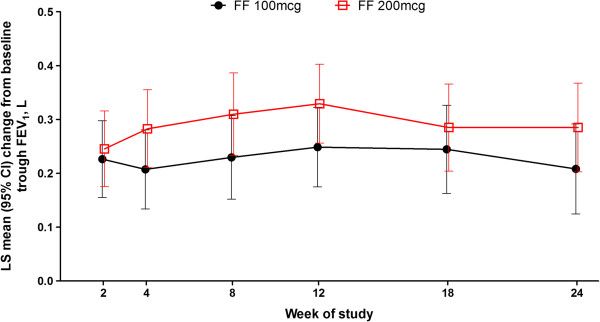
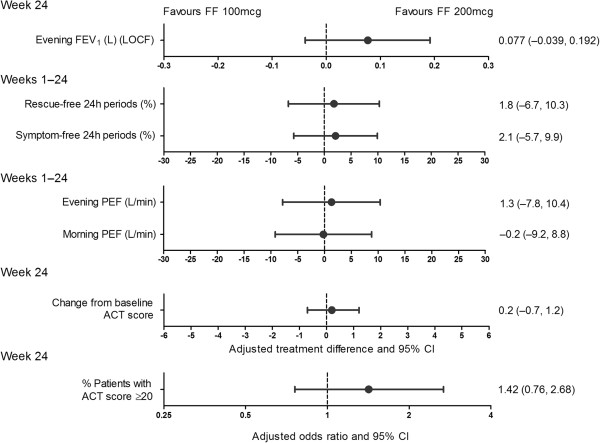
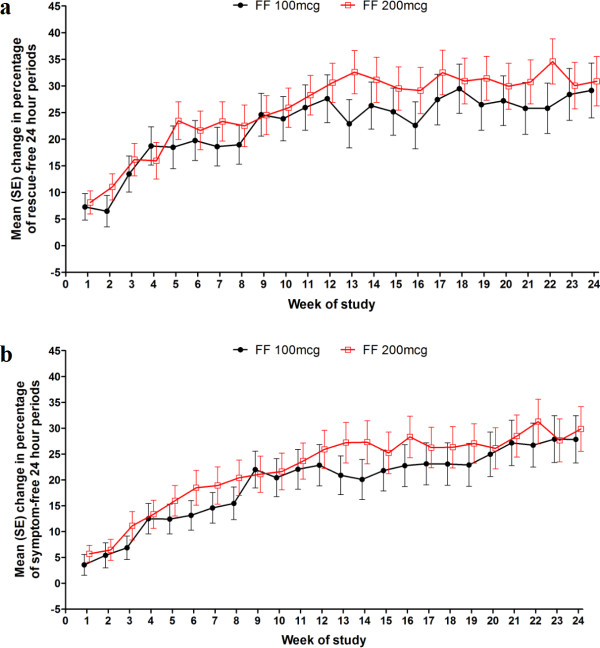
Results: With FF 100 μg and 200 μg, least squares mean trough FEV1 improved from baseline by 208 mL and 284 mL, respectively, at Week 24; treatment difference: 77 mL (95% CI: -39, 192). Similar improvements from baseline in rescue- and symptom-free periods, and morning and evening PEF were observed in both groups. Patients were 42% more likely to be well-controlled (ACT score ≥ 20) with FF 200 μg than with FF 100 μg. Slightly more patients receiving FF 200 μg vs. FF 100 μg reported adverse events (63% vs. 59%) and events deemed treatment related (5% vs. <1%). Seven serious adverse events (FF 200 μg 4; FF 100 μg 3) were reported, none of which were deemed treatment related. No clinically relevant effects of either dose on 24-hour urinary cortisol were observed.
Conclusion: Improvements from baseline in trough FEV1 were observed after 24 weeks of treatment with both doses of FF, with a numerically greater improvement in FEV1 observed in patients receiving FF 200 μg. Secondary endpoint findings were similar between groups. No safety concerns were identified during the study.
Figures
References
-
- Global Initiative for Asthma (GINA) Global Strategy for Asthma Management and Prevention. 2012. http://www.ginasthma.org/documents/5/documents_variants/37. Date last updated: December 2012. Date last accessed: 23 June 2014.
-
- Heaney LG, Horne R. Non-adherence in difficult asthma: time to take it seriously. Chest. 2012;67:268–270. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
