

Left ventricular geometric remodeling in relation to non-ischemic scar pattern on cardiac magnetic resonance imaging
- PMID: 25008088
- PMCID: PMC4233172
- DOI: 10.1007/s10554-014-0487-8
Left ventricular geometric remodeling in relation to non-ischemic scar pattern on cardiac magnetic resonance imaging
Abstract
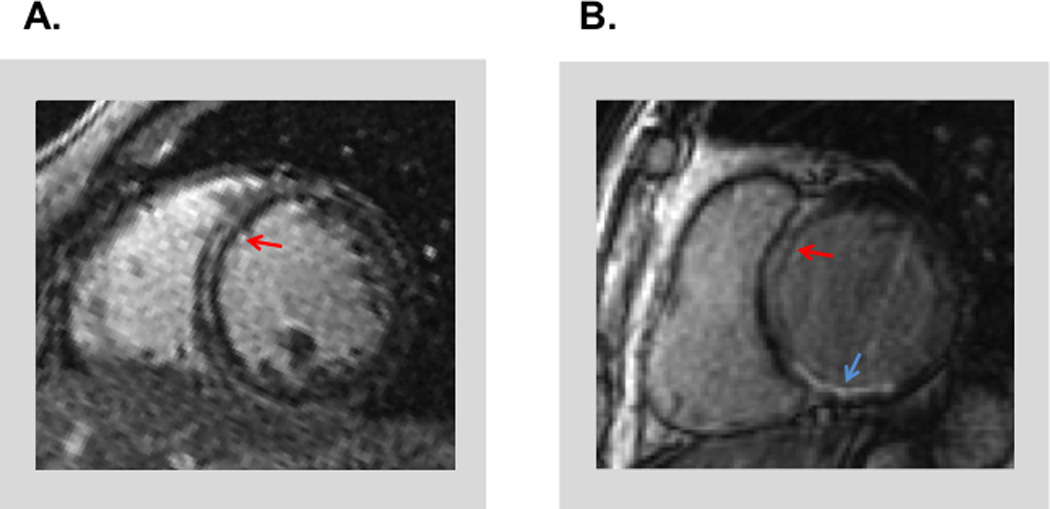
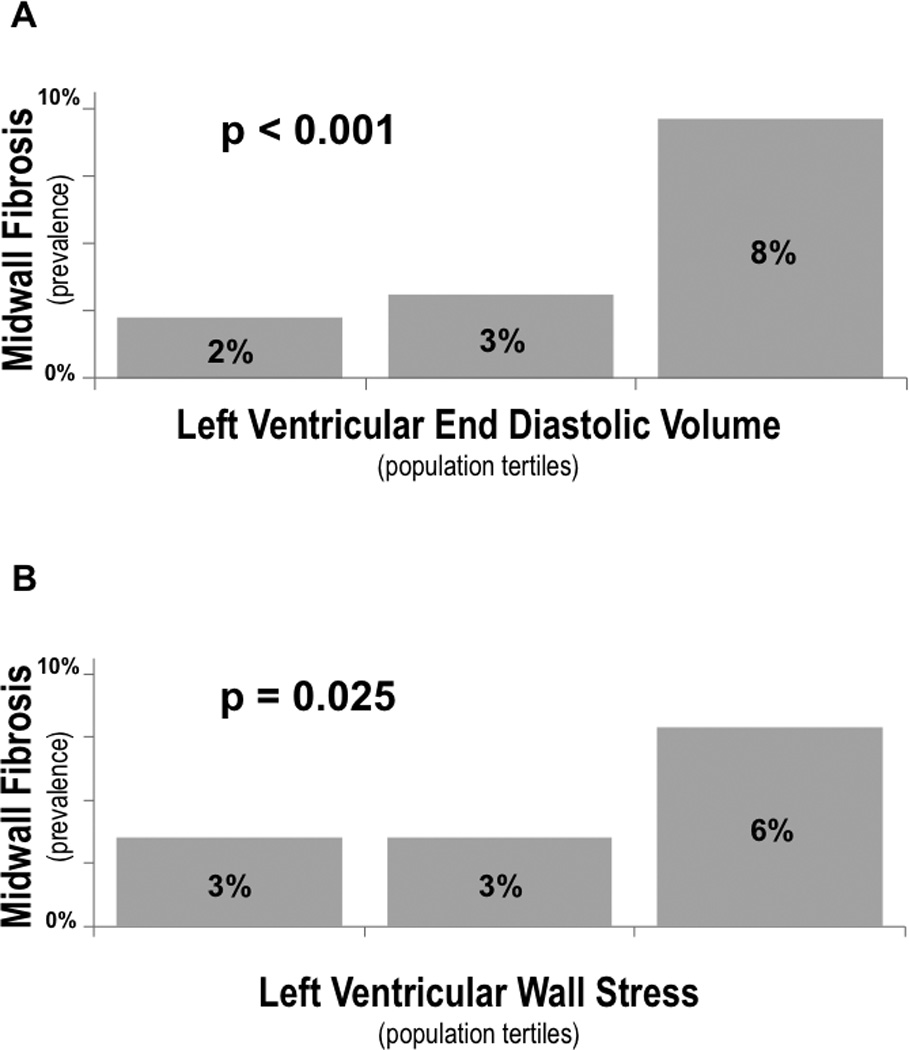
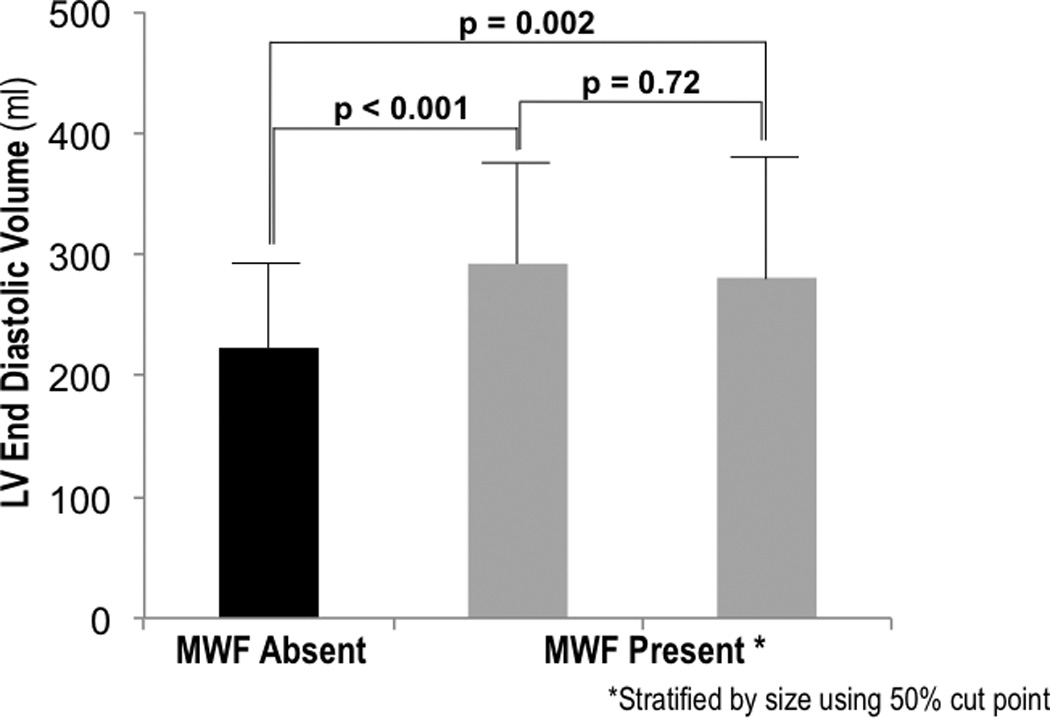
Left ventricular (LV) remodeling and myocardial fibrosis have been linked to adverse heart failure outcomes. Mid wall late gadolinium enhancement (MW-LGE) on cardiac magnetic resonance (CMR) imaging is well-associated with non-ischemic cardiomyopathy (NICM), but prevalence in ischemic cardiomyopathy (ICM) and association with remodeling are unknown. The population comprised patients with systolic dysfunction [LV ejection fraction (LVEF ≤ 40 %)]. CMR was used to identify MW-LGE, conventionally defined as fibrosis of the mid-myocardial or epicardial aspect of the LV septum. 285 patients were studied. MW-LGE was present in 12 %, and was tenfold more common with NICM (32 %) versus ICM (3 %, p < 0.001). However, owing to higher prevalence of ICM, 15 % of patients with MW-LGE had ICM. LV wall stress was higher (p = 0.02) among patients with, versus those without, MW-LGE despite similar systolic blood pressure (p = 0.24). In multivariate analysis, MW-LGE was associated with CMR-quantified LV end-diastolic volume (p = 0.03) independent of LVEF and mass. Incorporation of clinical and imaging variables demonstrated MW-LGE to be associated with higher LV end-diastolic volume (OR 1.13, CI 1.004-1.27 per 10 ml/m(2), p = 0.04) after controlling for presence of NICM (OR 16.0, CI 5.8-44.1, p < 0.001). While more common in NICM, MW-LGE can occur in ICM and is a marker of LV chamber dilation irrespective of cardiomyopathic etiology.
Conflict of interest statement
Figures
Comment in
-
Mystery of myocardial midwall late enhancement?Int J Cardiovasc Imaging. 2014 Dec;30(8):1569-70. doi: 10.1007/s10554-014-0514-9. Epub 2014 Aug 13. Int J Cardiovasc Imaging. 2014. PMID: 25117644 No abstract available.
References
-
- Migrino RQ, Young JB, Ellis SG, White HD, Lundergan CF, Miller DP, et al. End-systolic volume index at 90 to 180 minutes into reperfusion therapy for acute myocardial infarction is a strong predictor of early and late mortality. The Global Utilization of Streptokinase and t-PA for Occluded Coronary Arteries (GUSTO)-I Angiographic Investigators. Circulation. 1997;96:116–121. - PubMed
-
- Lee TH, Hamilton MA, Stevenson LW, Moriguchi JD, Fonarow GC, Child JS, et al. Impact of left ventricular cavity size on survival in advanced heart failure. Am J Cardiol. 1993;72:672–676. - PubMed
-
- Pfeffer MA, Braunwald E, Moyé LA, Basta L, Brown EJ, Cuddy TE, et al. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. Results of the survival and ventricular enlargement trial. The SAVE Investigators. N Engl J Med. 1992;327:669–677. - PubMed
-
- Sadoshima J, Xu Y, Slayter HS, Izumo S. Autocrine release of angiotensin II mediates stretch-induced hypertrophy of cardiac myocytes in vitro. Cell. 1993;75:977–984. - PubMed
-
- Harada K, Sugaya T, Murakami K, Yazaki Y, Komuro I. Angiotensin II type 1A receptor knockout mice display less left ventricular remodeling and improved survival after myocardial infarction. Circulation. 1999;100:2093–2099. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
