

Endogenous thrombin potential following hemostatic therapy with 4-factor prothrombin complex concentrate: a 7-day observational study of trauma patients
- PMID: 25008277
- PMCID: PMC4227066
- DOI: 10.1186/cc13982
Endogenous thrombin potential following hemostatic therapy with 4-factor prothrombin complex concentrate: a 7-day observational study of trauma patients
Abstract
Introduction: Purified prothrombin complex concentrate (PCC) is increasingly used as hemostatic therapy for trauma-induced coagulopathy (TIC). However, the impact of PCC administration on coagulation status among patients with TIC has not been adequately investigated.
Methods: In this observational, descriptive study, data relating to thrombin generation were obtained from plasma samples gathered prospectively from trauma patients upon emergency room (ER) admission and over the following 7 days. Standard coagulation tests, including measurement of antithrombin (AT) and fibrinogen, were performed. Three groups were investigated: patients receiving no coagulation therapy (NCT group), patients receiving fibrinogen concentrate only (FC group), and patients treated with PCC and fibrinogen concentrate (FC-PCC group).
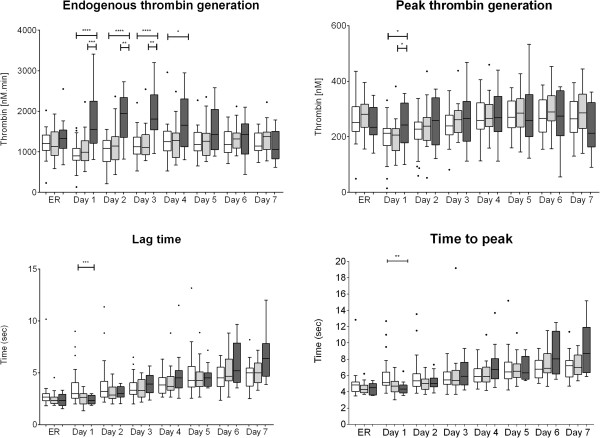
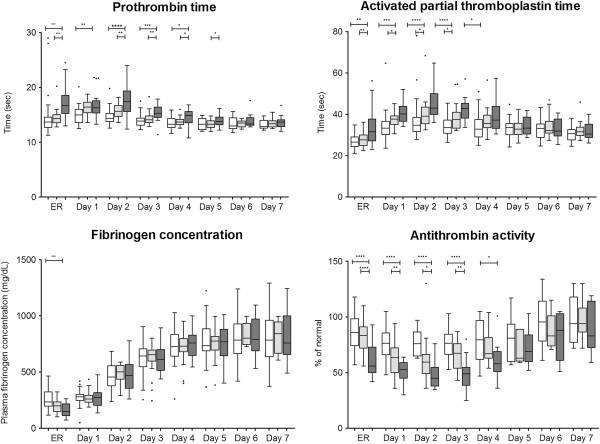
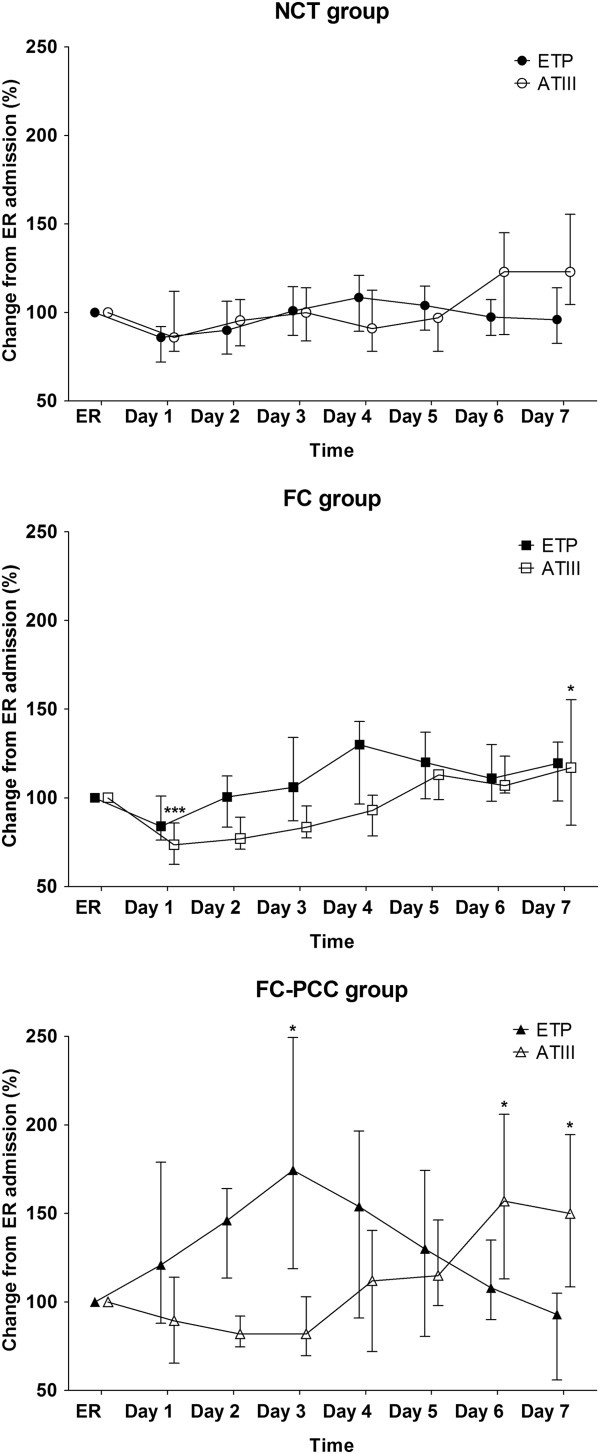
Results: The study population (77 patients) was predominantly male (84.4%); mean age was 40 ± 15 years and mean injury severity score was 25.6 ± 12.7. There were no significant differences between the three study groups in thrombin-related parameters upon ER admission. Endogenous thrombin potential (ETP) was significantly higher in the FC-PCC group compared with the NCT group on days 1 to 4 and the FC group on days 1 to 3. AT levels were significantly lower in the FC-PCC group from admission until day 3 (versus FC group) or day 4 (versus NCT group). Fibrinogen increased over time, with no significant between-group differences after ER admission. Despite ETP being higher, prothrombin time and activated partial thromboplastin time were significantly prolonged in the FC-PCC group from admission until day 3 to 4.
Conclusions: Treatment with PCC increased ETP for several days, and patients receiving PCC therapy had low AT concentrations. These findings imply a potential pro-thrombotic state not reflected by standard coagulation tests. This is probably important given the postoperative acute phase increase in fibrinogen levels, although studies with clinical endpoints are needed to ascertain the implications for patient outcomes. We recommend careful use of PCC among trauma patients, with monitoring and potentially supplementation of AT.
Figures
Similar articles
-
Impact of fibrinogen concentrate alone or with prothrombin complex concentrate (+/- fresh frozen plasma) on plasma fibrinogen level and fibrin-based clot strength (FIBTEM) in major trauma: a retrospective study.Scand J Trauma Resusc Emerg Med. 2013 Oct 8;21:74. doi: 10.1186/1757-7241-21-74. Scand J Trauma Resusc Emerg Med. 2013. PMID: 24103457 Free PMC article.
-
Hemostatic Therapy Using Tranexamic Acid and Coagulation Factor Concentrates in a Model of Traumatic Liver Injury.Anesth Analg. 2016 Jul;123(1):38-48. doi: 10.1213/ANE.0000000000001379. Anesth Analg. 2016. PMID: 27192476
-
Effect of coagulation factor concentrate administration on ROTEM® parameters in major trauma.Scand J Trauma Resusc Emerg Med. 2015 Oct 29;23:84. doi: 10.1186/s13049-015-0165-4. Scand J Trauma Resusc Emerg Med. 2015. PMID: 26514413 Free PMC article.
-
Restoring hemostasis with prothrombin complex concentrate: benefits and risks in trauma-induced coagulopathy.Curr Opin Anaesthesiol. 2025 Apr 1;38(2):120-128. doi: 10.1097/ACO.0000000000001464. Epub 2025 Feb 13. Curr Opin Anaesthesiol. 2025. PMID: 39937029 Review.
-
Prothrombin complex concentrate (PCC) for treatment of trauma-induced coagulopathy: systematic review and meta-analyses.Crit Care. 2023 Nov 2;27(1):422. doi: 10.1186/s13054-023-04688-z. Crit Care. 2023. PMID: 37919775 Free PMC article.
Cited by
-
[Individualized coagulation therapy: Wish or already reality?].Anaesthesist. 2015 Oct;64(10):727-9. doi: 10.1007/s00101-015-0059-x. Anaesthesist. 2015. PMID: 26194654 German. No abstract available.
-
[Management of hemorrhage in patients treated with direct oral anticoagulants].Anaesthesist. 2017 Sep;66(9):679-689. doi: 10.1007/s00101-017-0313-5. Anaesthesist. 2017. PMID: 28455651 Review. German.
-
Computational simulation and comparison of prothrombin complex concentrate dosing schemes for warfarin reversal in cardiac surgery.J Anesth. 2016 Jun;30(3):369-76. doi: 10.1007/s00540-015-2128-3. Epub 2016 Jan 9. J Anesth. 2016. PMID: 26749482
-
Retrospective Review of a Prothrombin Complex Concentrate (Beriplex P/N) for the Management of Perioperative Bleeding Unrelated to Oral Anticoagulation.Clin Appl Thromb Hemost. 2018 Oct;24(7):1159-1169. doi: 10.1177/1076029617753537. Epub 2018 Feb 7. Clin Appl Thromb Hemost. 2018. PMID: 29415562 Free PMC article. Review.
-
Inhospital coagulation management and fluid replacement therapy in patients with multiple and/or severe injuries - a systematic review and clinical practice guideline update.Eur J Trauma Emerg Surg. 2025 Jun 27;51(1):240. doi: 10.1007/s00068-025-02919-2. Eur J Trauma Emerg Surg. 2025. PMID: 40576680 Free PMC article.
References
-
- Johansson PI, Sørensen AM, Larsen CF, Windeløv NA, Stensballe J, Perner A, Rasmussen LS, Ostrowski SR. Low hemorrhage-related mortality in trauma patients in a Level I trauma center employing transfusion packages and early thromboelastography-directed hemostatic resuscitation with plasma and platelets. Transfusion. 2013;53:3088–3099. doi: 10.1111/trf.12214. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
