

Laparoscopic vs open approach to resection of hepatocellular carcinoma in patients with known cirrhosis: systematic review and meta-analysis
- PMID: 25009403
- PMCID: PMC4081703
- DOI: 10.3748/wjg.v20.i25.8274
Laparoscopic vs open approach to resection of hepatocellular carcinoma in patients with known cirrhosis: systematic review and meta-analysis
Abstract
Aim: To review the currently available literature comparing laparoscopic to open resection of hepatocellular carcinoma (HCC) in patients with known liver cirrhosis.
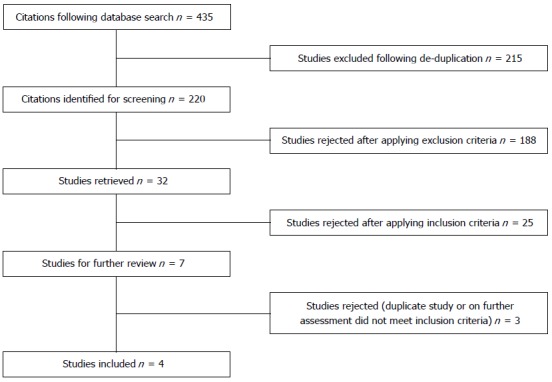
Methods: A literature search of MEDLINE, EMBASE, and Cochrane databases was conducted. The search terms used included (laparoscopic OR laparoscopy) AND (hepatic or liver) AND (surgery or resection) AND "hepatocellular carcinoma" AND (cirrhosis or cirrhotic). Furthermore, to widen the search, we also used the "related articles" section. Studies reporting a comparison of outcomes and methods of open vs laparoscopic hepatic resection for HCC in patients with liver cirrhosis were included. Meta-analysis of results was performed using a random effects model to compute relative risk (RR) and for dichotomous variables and standard mean differences (SMD) for continuous variables.
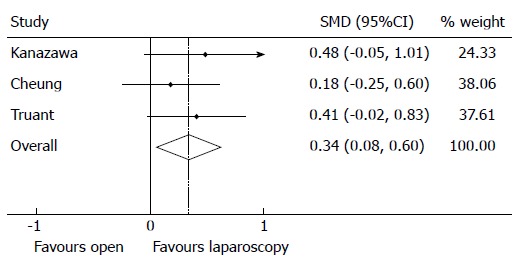
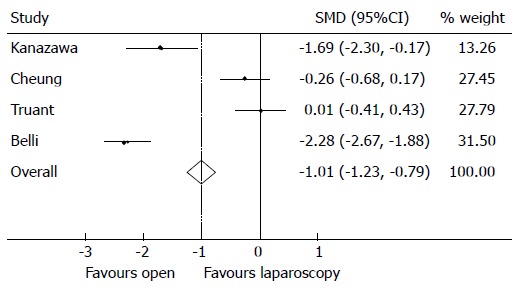
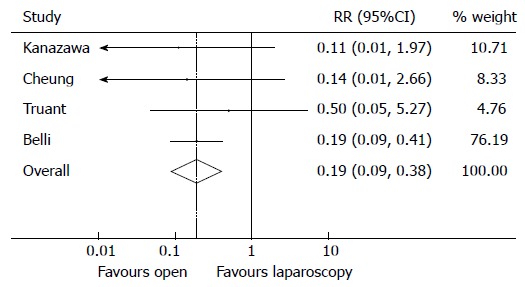
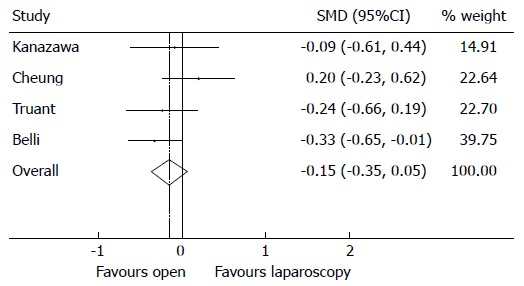
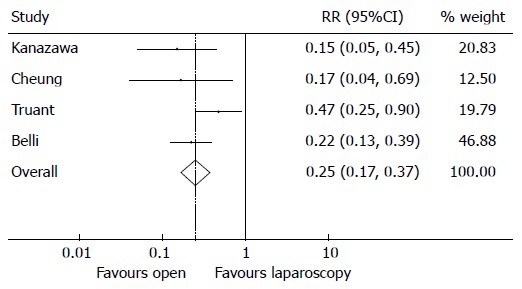
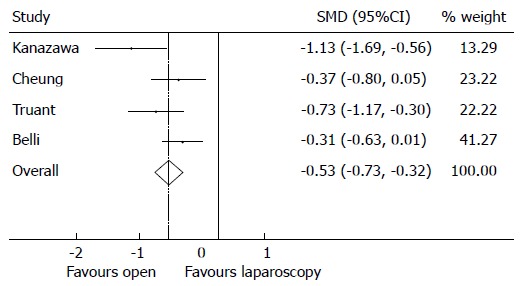
Results: A total of 420 patients from 4 cohort studies were included in final analysis. Patients undergoing laparoscopic procedures had statistically less blood loss compared to the open cohort, SMD of -1.01 (95%CI: -1.23-0.79), P < 0.001, with a reduced risk of transfusion, RR = 0.19 (95%CI: 0.09-0.38), P < 0.001. A wider clearance at tumour resection margins was achieved following a laparoscopic approach, SMD of 0.34 (95%CI: 0.08-0.60), P = 0.011. No significant difference was noted between laparoscopic and open resection operative times, SMD of -0.15 (95%CI: 0.35-0.05), P = 0.142. The overall RR of suffering from postoperative morbidity is 0.25 in favour of the open surgery cohort (95%CI: 0.17-0.37), P < 0.001. Patients under-going laparoscopic surgery had significantly shorter length of stays in hospital compared to the open cohort, SMD of -0.53 (95%CI: -0.73 to -0.32), P < 0.001.
Conclusion: This review suggests that laparoscopic resection of hepatocellular carcinoma in patients with cirrhosis is safe and may provide improved patient outcomes when compared to the open technique.
Keywords: Cirrhosis; Hepatic resection; Hepatobiliary; Hepatocellular carcinoma; Laparoscopic; Surgery; Surgical oncology.
Figures
Comment in
-
Re: ''laparoscopic vs open approach to resection of hepatocellular carcinoma in patients with known cirrhosis: systematic review and meta-analysis''.World J Gastroenterol. 2015 Jan 7;21(1):377-8. doi: 10.3748/wjg.v21.i1.377. World J Gastroenterol. 2015. PMID: 25574115 Free PMC article.
References
-
- Veldkamp R, Kuhry E, Hop WC, Jeekel J, Kazemier G, Bonjer HJ, Haglind E, Påhlman L, Cuesta MA, Msika S, et al. Laparoscopic surgery versus open surgery for colon cancer: short-term outcomes of a randomised trial. Lancet Oncol. 2005;6:477–484. - PubMed
-
- Berggren U, Gordh T, Grama D, Haglund U, Rastad J, Arvidsson D. Laparoscopic versus open cholecystectomy: hospitalization, sick leave, analgesia and trauma responses. Br J Surg. 1994;81:1362–1365. - PubMed
-
- Golub R, Siddiqui F, Pohl D. Laparoscopic versus open appendectomy: a metaanalysis. J Am Coll Surg. 1998;186:545–553. - PubMed
-
- Peters MJ, Mukhtar A, Yunus RM, Khan S, Pappalardo J, Memon B, Memon MA. Meta-analysis of randomized clinical trials comparing open and laparoscopic anti-reflux surgery. Am J Gastroenterol. 2009;104:1548–1561; quiz 1547, 1562. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
