

Single-subject-based whole-brain MEG slow-wave imaging approach for detecting abnormality in patients with mild traumatic brain injury
- PMID: 25009772
- PMCID: PMC4087185
- DOI: 10.1016/j.nicl.2014.06.004
Single-subject-based whole-brain MEG slow-wave imaging approach for detecting abnormality in patients with mild traumatic brain injury
Abstract
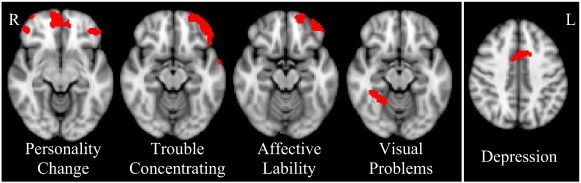
Traumatic brain injury (TBI) is a leading cause of sustained impairment in military and civilian populations. However, mild TBI (mTBI) can be difficult to detect using conventional MRI or CT. Injured brain tissues in mTBI patients generate abnormal slow-waves (1-4 Hz) that can be measured and localized by resting-state magnetoencephalography (MEG). In this study, we develop a voxel-based whole-brain MEG slow-wave imaging approach for detecting abnormality in patients with mTBI on a single-subject basis. A normative database of resting-state MEG source magnitude images (1-4 Hz) from 79 healthy control subjects was established for all brain voxels. The high-resolution MEG source magnitude images were obtained by our recent Fast-VESTAL method. In 84 mTBI patients with persistent post-concussive symptoms (36 from blasts, and 48 from non-blast causes), our method detected abnormalities at the positive detection rates of 84.5%, 86.1%, and 83.3% for the combined (blast-induced plus with non-blast causes), blast, and non-blast mTBI groups, respectively. We found that prefrontal, posterior parietal, inferior temporal, hippocampus, and cerebella areas were particularly vulnerable to head trauma. The result also showed that MEG slow-wave generation in prefrontal areas positively correlated with personality change, trouble concentrating, affective lability, and depression symptoms. Discussion is provided regarding the neuronal mechanisms of MEG slow-wave generation due to deafferentation caused by axonal injury and/or blockages/limitations of cholinergic transmission in TBI. This study provides an effective way for using MEG slow-wave source imaging to localize affected areas and supports MEG as a tool for assisting the diagnosis of mTBI.
Keywords: Axonal injury; Blast; Magnetoencephalography; Slow-wave; Traumatic brain injury.
Figures




Similar articles
-
An automatic MEG low-frequency source imaging approach for detecting injuries in mild and moderate TBI patients with blast and non-blast causes.Neuroimage. 2012 Jul 16;61(4):1067-82. doi: 10.1016/j.neuroimage.2012.04.029. Epub 2012 Apr 20. Neuroimage. 2012. PMID: 22542638
-
The role of biomarkers and MEG-based imaging markers in the diagnosis of post-traumatic stress disorder and blast-induced mild traumatic brain injury.Psychoneuroendocrinology. 2016 Jan;63:398-409. doi: 10.1016/j.psyneuen.2015.02.008. Epub 2015 Feb 23. Psychoneuroendocrinology. 2016. PMID: 25769625
-
Integrated imaging approach with MEG and DTI to detect mild traumatic brain injury in military and civilian patients.J Neurotrauma. 2009 Aug;26(8):1213-26. doi: 10.1089/neu.2008.0672. J Neurotrauma. 2009. PMID: 19385722
-
[Mild traumatic brain injury and postconcussive syndrome: a re-emergent questioning].Encephale. 2012 Sep;38(4):329-35. doi: 10.1016/j.encep.2011.07.003. Epub 2011 Aug 31. Encephale. 2012. PMID: 22980474 Review. French.
-
Magnetoencephalography in the diagnosis of concussion.Prog Neurol Surg. 2014;28:94-111. doi: 10.1159/000358768. Epub 2014 Jun 6. Prog Neurol Surg. 2014. PMID: 24923396 Review.
Cited by
-
Emerging Approaches to Neurocircuits in PTSD and TBI: Imaging the Interplay of Neural and Emotional Trauma.Curr Top Behav Neurosci. 2018;38:163-192. doi: 10.1007/7854_2017_35. Curr Top Behav Neurosci. 2018. PMID: 29285732 Free PMC article. Review.
-
Neuroimaging findings and balance problems after mild traumatic brain injury: A systematic review protocol.PLoS One. 2025 Feb 5;20(2):e0307339. doi: 10.1371/journal.pone.0307339. eCollection 2025. PLoS One. 2025. PMID: 39908314 Free PMC article.
-
Mild traumatic brain injury is associated with dysregulated neural network functioning in children and adolescents.Brain Commun. 2021 Mar 17;3(2):fcab044. doi: 10.1093/braincomms/fcab044. eCollection 2021. Brain Commun. 2021. PMID: 34095832 Free PMC article.
-
Traumatic brain injury imaging research roadmap.AJNR Am J Neuroradiol. 2015 Mar;36(3):E12-23. doi: 10.3174/ajnr.A4254. Epub 2015 Feb 5. AJNR Am J Neuroradiol. 2015. PMID: 25655872 Free PMC article. Review.
-
Alpha desynchronization/synchronization during working memory testing is compromised in acute mild traumatic brain injury (mTBI).PLoS One. 2018 Feb 14;13(2):e0188101. doi: 10.1371/journal.pone.0188101. eCollection 2018. PLoS One. 2018. PMID: 29444081 Free PMC article.
References
-
- Adams J.H., Doyle D., Ford I., Gennarelli T.A., Graham D.I., McLellan D.R. Diffuse axonal injury in head injury: definition, diagnosis and grading. Histopathology. 1989;15:49–59. - PubMed
-
- Alexander M.P. Mild traumatic brain injury: pathophysiology, natural history, and clinical management. Neurology. 1995;45:1253–1260. - PubMed
-
- Babbage D.R., Yim J., Zupan B., Neumann D., Tomita M.R., Willer B. Meta-analysis of facial affect recognition difficulties after traumatic brain injury. Neuropsychology. 2011;25:277–285. - PubMed
-
- Ball G.J., Gloor P., Schaul N. The cortical electromicrophysiology of pathological delta waves in the electroencephalogram of cats. Electroencephalogr. Clin. Neurophysiol. 1977;43:346–361. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
