

Microincision vitrectomy surgery in vitreomacular traction syndrome of retinitis pigmentosa patients
- PMID: 25009817
- PMCID: PMC4070290
- DOI: 10.1155/2014/537081
Microincision vitrectomy surgery in vitreomacular traction syndrome of retinitis pigmentosa patients
Abstract
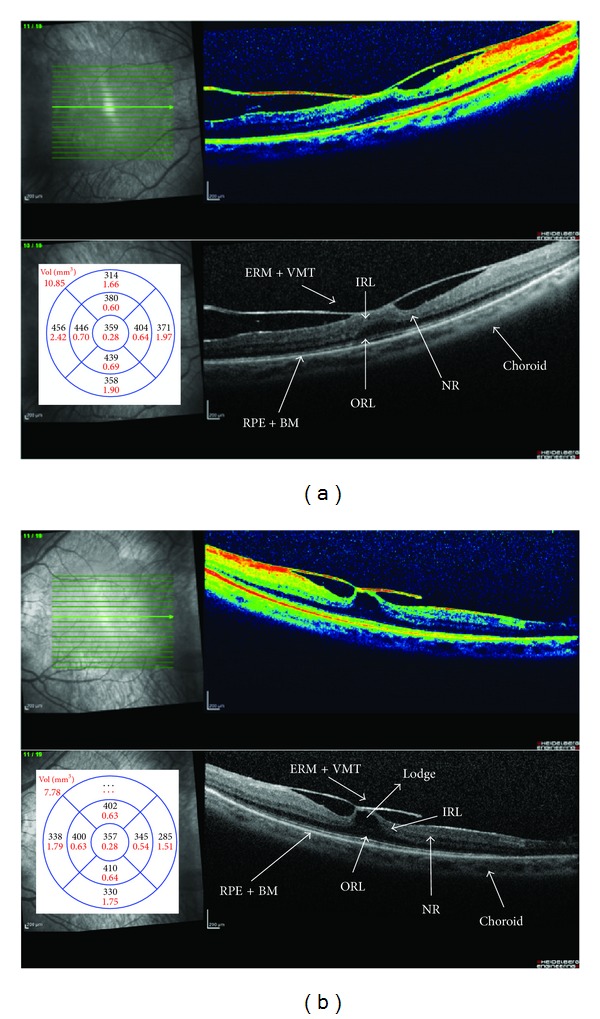
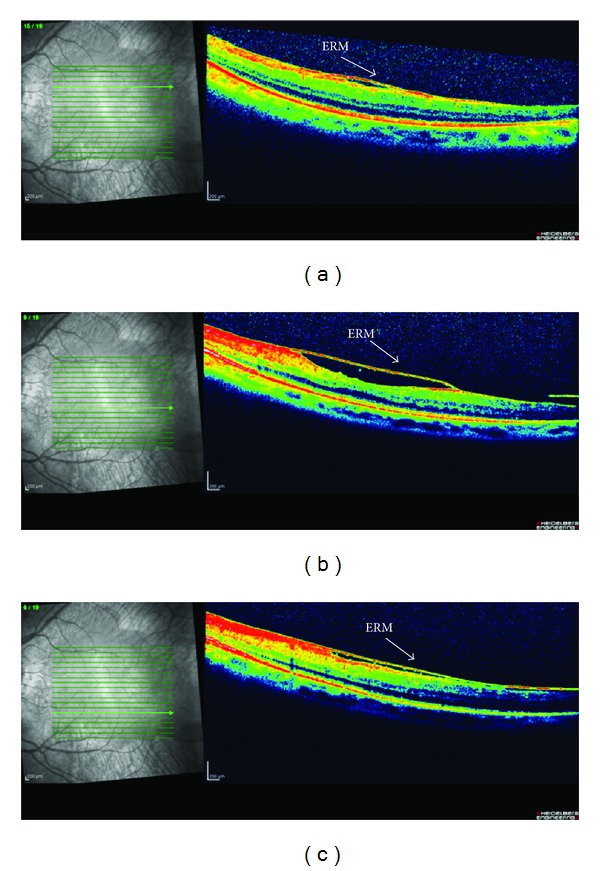
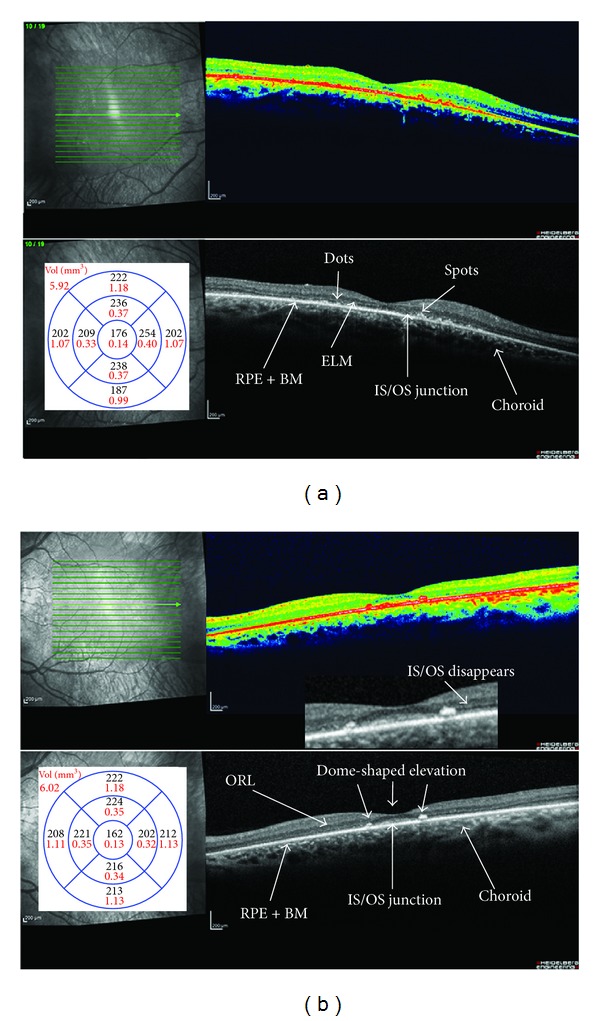
Purpose: To investigate long-term retinal changes after microincision pars plana vitrectomy surgery (MIVS) and internal limiting membrane (ILM) peeling outcome in retinitis pigmentosa (RP) patients affected by vitreomacular traction syndrome (VMT) with higher vitreous surface adhesion or coexisting epiretinal membrane (ERM).
Methods: Eight RP patients suffering from VMT were evaluated by means of best corrected visual acuity (BCVA), anterior and posterior binocular examination, spectral-domain optical coherence tomography (SD-OCT), MP-1 microperimetry (MP-1), and full-field electroretinogram (ERG), before MIVS and ILM peeling and during the 36-month follow-up. Patients were hospitalized for two days after the surgery. Surgical procedure was performed following this schedule: surgical removal of crystalline lens (MICS), MIVS with 23-gauge sutureless system trocars, core vitreous body removal, and balanced-sterile-salin-solution- (BSS-) air-gas (SF6) exchange.
Results: All patients presented visual acuity (VA) increase after MIVS. None of the patients developed ocular hypertension or vitreomacular adhesions during the 3-year follow-up. MP-1 bivariate contour ellipse area (BCEA) was reduced in its dimensions and improved in all patients demonstrating a better fixation.
Conclusions: MIVS could be the gold standard therapy in RP patients with VMT and higher vitreous surface adhesion or coexisting ERM if medical therapy is not applicable or not effective.
Figures
References
-
- Griever S, Fishman GA, Anderson RJ, Alexander KR, Derlacki DJ. Rate of visual field loss in retinitis pigmentosa. Ophthalmology. 1997;104(3):460–465. - PubMed
-
- Berson EL. Retinitis pigmentosa: the Friedenwald lecture. Investigative Ophthalmology and Visual Science. 1993;34(5):1659–1676. - PubMed
-
- Hajali M, Fishman GA, Anderson RJ. The prevalence of cystoid macular oedema in retinitis pigmentosa patients determined by optical coherence tomography. British Journal of Ophthalmology. 2008;92(8):1065–1068. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
