

Loss to clinic and five-year mortality among HIV-infected antiretroviral therapy initiators
- PMID: 25010739
- PMCID: PMC4092142
- DOI: 10.1371/journal.pone.0102305
Loss to clinic and five-year mortality among HIV-infected antiretroviral therapy initiators
Abstract
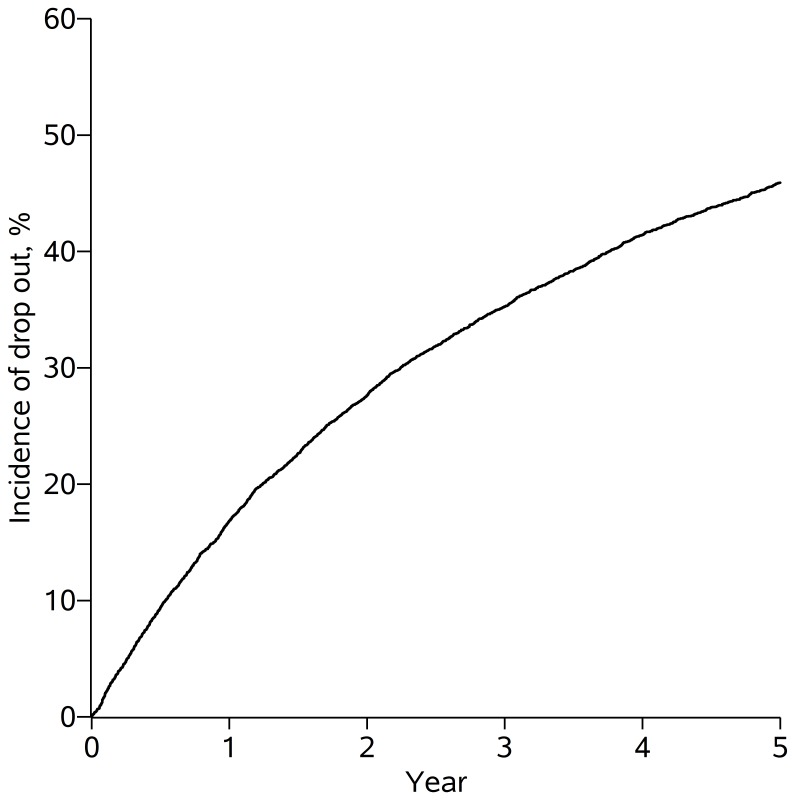
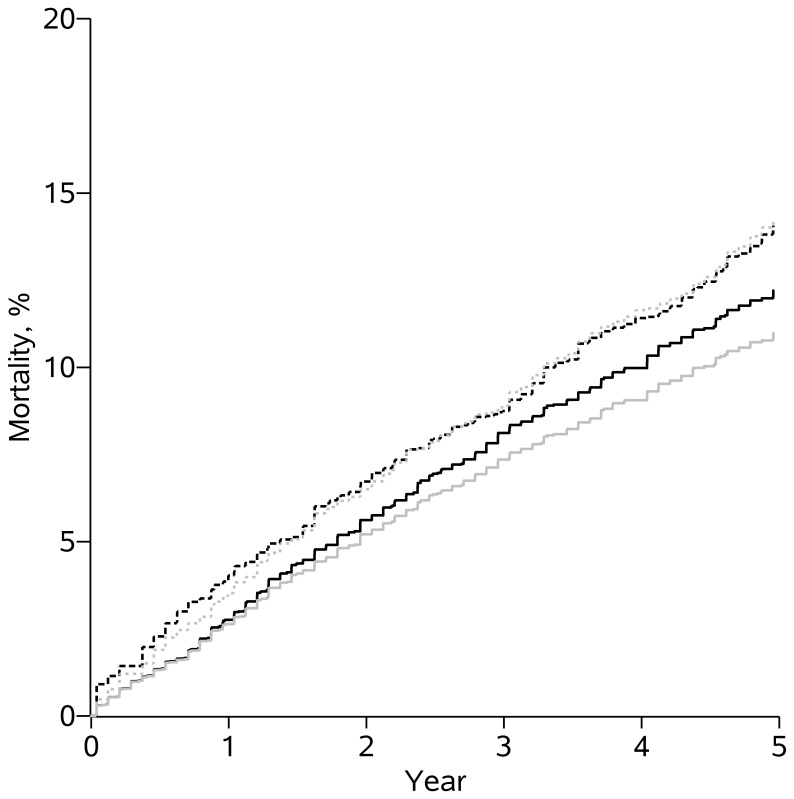
Missing outcome data due to loss to follow-up occurs frequently in clinical cohort studies of HIV-infected patients. Censoring patients when they become lost can produce inaccurate results if the risk of the outcome among the censored patients differs from the risk of the outcome among patients remaining under observation. We examine whether patients who are considered lost to follow up are at increased risk of mortality compared to those who remain under observation. Patients from the US Centers for AIDS Research Network of Integrated Clinical Systems (CNICS) who newly initiated combination antiretroviral therapy between January 1, 1998 and December 31, 2009 and survived for at least one year were included in the study. Mortality information was available for all participants regardless of continued observation in the CNICS. We compare mortality between patients retained in the cohort and those lost-to-clinic, as commonly defined by a 12-month gap in care. Patients who were considered lost-to-clinic had modestly elevated mortality compared to patients who remained under observation after 5 years (risk ratio (RR): 1.2; 95% CI: 0.9, 1.5). Results were similar after redefining loss-to-clinic as 6 months (RR: 1.0; 95% CI: 0.8, 1.3) or 18 months (RR: 1.2; 95% CI: 0.8, 1.6) without a documented clinic visit. The small increase in mortality associated with becoming lost to clinic suggests that these patients were not lost to care, rather they likely transitioned to care at a facility outside the study. The modestly higher mortality among patients who were lost-to-clinic implies that when we necessarily censor these patients in studies of time-varying exposures, we are likely to incur at most a modest selection bias.
Conflict of interest statement
Figures
References
-
- Klein JP, Moeschberger ML (2005) Survival Analysis: Techniques for Censored and Truncated Data. Springer; 2nd edition.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
