

Alerting thresholds for the prevention of intraoperative awareness with explicit recall: a secondary analysis of the Michigan Awareness Control Study
- PMID: 25010744
- PMCID: PMC4737525
- DOI: 10.1097/EJA.0000000000000123
Alerting thresholds for the prevention of intraoperative awareness with explicit recall: a secondary analysis of the Michigan Awareness Control Study
Abstract
Background: Intraoperative awareness with explicit recall is a potentially devastating complication of surgery that has been attributed to low anaesthetic concentrations in the vast majority of cases. Past studies have proposed the determination of an adequate dose for general anaesthetics that could be used to alert providers of potentially insufficient anaesthesia. However, there have been no systematic analyses of appropriate thresholds to develop population-based alerting algorithms for preventing intraoperative awareness.
Objective: To identify a threshold for intraoperative alerting that could be applied for the prevention of awareness with explicit recall.
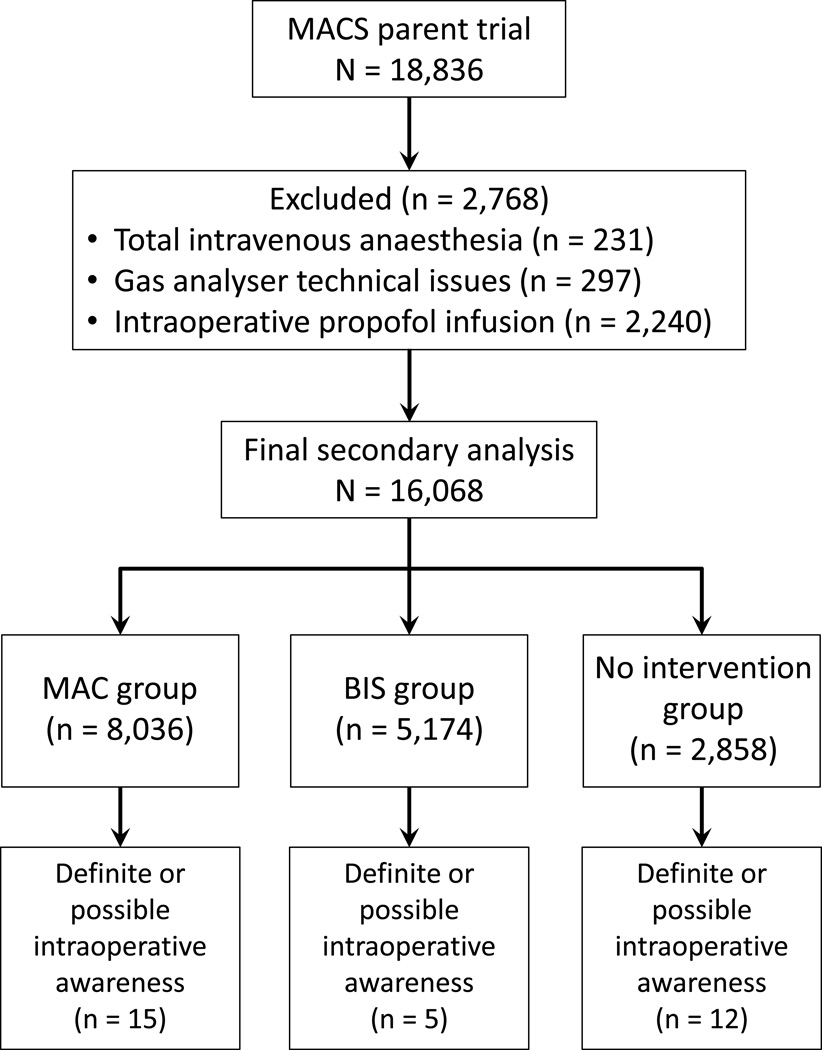
Design: Secondary analysis of a randomised controlled trial (Michigan Awareness Control Study).
Setting: Three hospitals at a tertiary care centre in the USA.
Patients: Unselected patients presenting for surgery under general anaesthesia.
Interventions: Alerts based on end-tidal anaesthetic concentration or bispectral index values.
Main outcome measures: Using case and outcomes data from the primary study, end-tidal anaesthetic concentration and bispectral index values were analysed using Youden's index and c-statistics derived from a receiver operating characteristic curve to determine a specific alerting threshold for the prevention of awareness.
Results: No single population-based threshold that maximises sensitivity and specificity could be identified for the prevention of intraoperative awareness, using either anaesthetic concentration or bispectral index values. The c-statistic for anaesthetic concentration was 0.431 ± 0.046, and 0.491 ± 0.056 for bispectral index values.
Conclusion: We could not derive a single population-based alerting threshold for the prevention of intraoperative awareness using either anaesthetic concentration or bispectral index values. These data indicate a need to move towards individualised alerting strategies in the prevention of intraoperative awareness.
Trial registration: Primary trial registration (Michigan Awareness Control Study) ClinicalTrials.gov identifier: NCT00689091.
Conflict of interest statement
Conflicts of interest: G.A.M. has a patent pending (through the University of Michigan) on the use of connectivity measures to assess levels of consciousness.
Figures
Comment in
-
Bispectral index aware or minimum alveolar concentration aware?: Alerting thresholds for prevention of awareness.Eur J Anaesthesiol. 2015 May;32(5):301-2. doi: 10.1097/EJA.0000000000000199. Eur J Anaesthesiol. 2015. PMID: 25840347 No abstract available.
References
-
- Moerman N, Bonke B, Oosting J. Awareness and recall during general anesthesia. Facts and feelings. Anesthesiology. 1993;79:454–464. - PubMed
-
- Schwender D, Kunze-Kronawitter H, Dietrich P, Klasing S, Forst H, Madler C. Conscious awareness during general anaesthesia: patients' perceptions, emotions, cognition and reactions. Br J Anaesth. 1998;80:133–139. - PubMed
-
- Domino KB, Posner KL, Caplan RA, Cheney FW. Awareness during anesthesia: a closed claims analysis. Anesthesiology. 1999;90:1053–1061. - PubMed
-
- Osterman JE, Hopper J, Heran WJ, Keane TM, van der Kolk BA. Awareness under anesthesia and the development of posttraumatic stress disorder. Gen Hosp Psychiatry. 2001;23:198–204. - PubMed
-
- Ghoneim MM, Block RI, Haffarnan M, Mathews MJ. Awareness during anesthesia: risk factors, causes and sequelae: a review of reported cases in the literature. Anesth Analg. 2009;108:527–535. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
