

Indomethacin, amiloride, or eplerenone for treating hypokalemia in Gitelman syndrome
- PMID: 25012174
- PMCID: PMC4310664
- DOI: 10.1681/ASN.2014030293
Indomethacin, amiloride, or eplerenone for treating hypokalemia in Gitelman syndrome
Abstract
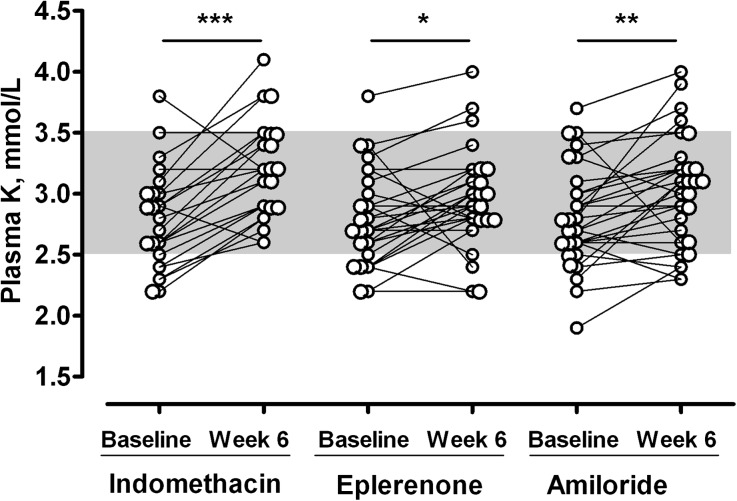
Patients with Gitelman syndrome (GS), an inherited salt-losing tubulopathy, are usually treated with potassium-sparing diuretics or nonsteroidal anti-inflammatory drugs and oral potassium and magnesium supplementations. However, evidence supporting these treatment options is limited to case series studies. We designed an open-label, randomized, crossover study with blind end point evaluation to compare the efficacy and safety of 6-week treatments with one time daily 75 mg slow-release indomethacin, 150 mg eplerenone, or 20 mg amiloride added to constant potassium and magnesium supplementation in 30 patients with GS (individual participation: 48 weeks). Baseline plasma potassium concentration was 2.8±0.4 mmol/L and increased by 0.38 mmol/L (95% confidence interval [95% CI], 0.23 to 0.53; P<0.001) with indomethacin, 0.15 mmol/L (95% CI, 0.02 to 0.29; P=0.03) with eplerenone, and 0.19 mmol/L (95% CI, 0.05 to 0.33; P<0.01) with amiloride. Fifteen patients became normokalemic: six with indomethacin, three with eplerenone, and six with amiloride. Indomethacin significantly reduced eGFR and plasma renin concentration. Eplerenone and amiloride each increased plasma aldosterone by 3-fold and renin concentration slightly but did not significantly change eGFR. BP did not significantly change. Eight patients discontinued treatment early because of gastrointestinal intolerance to indomethacin (six patients) and hypotension with eplerenone (two patients). In conclusion, each drug increases plasma potassium concentration in patients with GS. Indomethacin was the most effective but can cause gastrointestinal intolerance and decreased eGFR. Amiloride and eplerenone have similar but lower efficacies and increase sodium depletion. The benefit/risk ratio of each drug should be carefully evaluated for each patient.
Keywords: Gitelman syndrome; distal tubule; diuretics.
Copyright © 2015 by the American Society of Nephrology.
Figures
References
-
- Simon DB, Nelson-Williams C, Bia MJ, Ellison D, Karet FE, Molina AM, Vaara I, Iwata F, Cushner HM, Koolen M, Gainza FJ, Gitleman HJ, Lifton RP: Gitelman’s variant of Bartter’s syndrome, inherited hypokalaemic alkalosis, is caused by mutations in the thiazide-sensitive Na-Cl cotransporter. Nat Genet 12: 24–30, 1996 - PubMed
-
- Malafronte C, Borsa N, Tedeschi S, Syrèn ML, Stucchi S, Bianchetti MG, Achilli F, Bettinelli A: Cardiac arrhythmias due to severe hypokalemia in a patient with classic Bartter disease. Pediatr Nephrol 19: 1413–1415, 2004 - PubMed
-
- Ahmed S, Qayyum M, Farooq F: Quadriparesis in an adult—Gitelman syndrome. J Pak Med Assoc 61: 182–184, 2011 - PubMed
-
- Scognamiglio R, Negut C, Calò LA: Aborted sudden cardiac death in two patients with Bartter’s/Gitelman’s syndromes. Clin Nephrol 67: 193–197, 2007 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
