

Outcome of corneal collagen crosslinking for progressive keratoconus in paediatric patients
- PMID: 25013757
- PMCID: PMC4071785
- DOI: 10.1155/2014/140461
Outcome of corneal collagen crosslinking for progressive keratoconus in paediatric patients
Abstract
Purpose: To evaluate the efficacy of corneal collagen crosslinking for progressive keratoconus in paediatric patients.
Methods: This prospective study included 25 eyes of 18 patients (aged 18 years or younger) who underwent collagen crosslinking performed using riboflavin and ultraviolet-A irradiation (370 nm, 3 mW/cm2, 30 min).
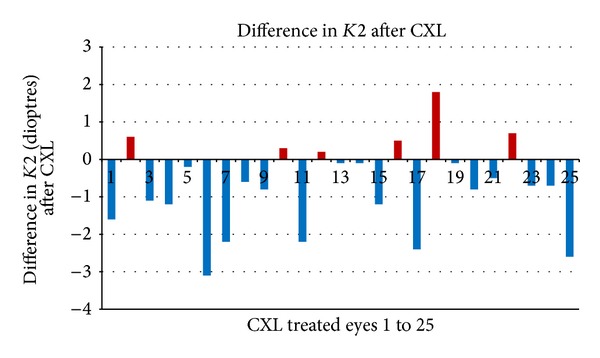
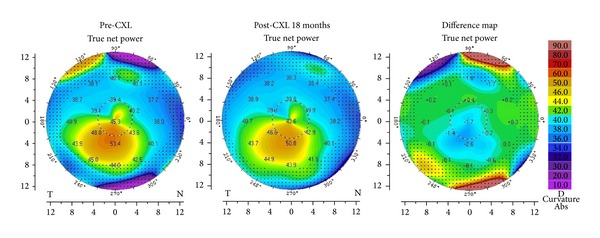
Results: The mean patient age was 14.3±2.4 years (range 8-17) and mean followup duration was 20.1±14.25 months (range 6-48). Crosslinked eyes demonstrated a significant reduction of keratometry values. The mean baseline simulated keratometry values were 46.34 dioptres (D) in the flattest meridian and 50.06 D in the steepest meridian. At 20 months after crosslinking, the values were 45.67 D (P=0.03) and 49.34 D (P=0.005), respectively. The best spectacle corrected visual acuity (BSCVA) and topometric astigmatism improved after crosslinking. Mean logarithm of the minimum angle of resolution (logMAR) BSCVA decreased from 0.24 to 0.21 (P=0.89) and topometric astigmatism reduced from mean 3.50 D to 3.25 D (P=0.51).
Conclusions: Collagen crosslinking using riboflavin and ultraviolet-A is an effective treatment option for progressive keratoconus in paediatric patients. Crosslinking stabilises the condition and, thus, reduces the need for corneal grafting in these young patients.
Figures
References
-
- Rabinowitz YS. Keratoconus. Survey of Ophthalmology. 1998;42(4):297–319. - PubMed
-
- Edmund C. Assessment of an elastic model in the pathogenesis of keratoconus. Acta Ophthalmologica. 1987;65(5):545–550. - PubMed
-
- Reeves SW, Stinnett S, Adelman RA, Afshari NA. Risk factors for progression to penetrating keratoplasty in patients with keratoconus. American Journal of Ophthalmology. 2005;140(4):607–611. - PubMed
-
- Spoerl E, Wollensak G, Seiler T. Increased resistance of crosslinked cornea against enzymatic digestion. Current Eye Research. 2004;29(1):35–40. - PubMed
-
- Kohlhaas M, Spoerl E, Schilde T, Unger G, Wittig C, Pillunat LE. Biomechanical evidence of the distribution of cross-links in corneastreated with riboflavin and ultraviolet a light. Journal of Cataract and Refractive Surgery. 2006;32(2):279–283. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
