

Safety and tolerability of once-daily umeclidinium/vilanterol 125/25 mcg and umeclidinium 125 mcg in patients with chronic obstructive pulmonary disease: results from a 52-week, randomized, double-blind, placebo-controlled study
- PMID: 25015176
- PMCID: PMC4113670
- DOI: 10.1186/1465-9921-15-78
Safety and tolerability of once-daily umeclidinium/vilanterol 125/25 mcg and umeclidinium 125 mcg in patients with chronic obstructive pulmonary disease: results from a 52-week, randomized, double-blind, placebo-controlled study
Abstract
Background: The long-acting muscarinic antagonist (LAMA) umeclidinium (UMEC) and the combination of UMEC with the long-acting β2-agonist (LABA) vilanterol (UMEC/VI) are approved maintenance treatments for chronic obstructive pulmonary disease (COPD) in the US and EU. They are not indicated for the treatment of asthma.
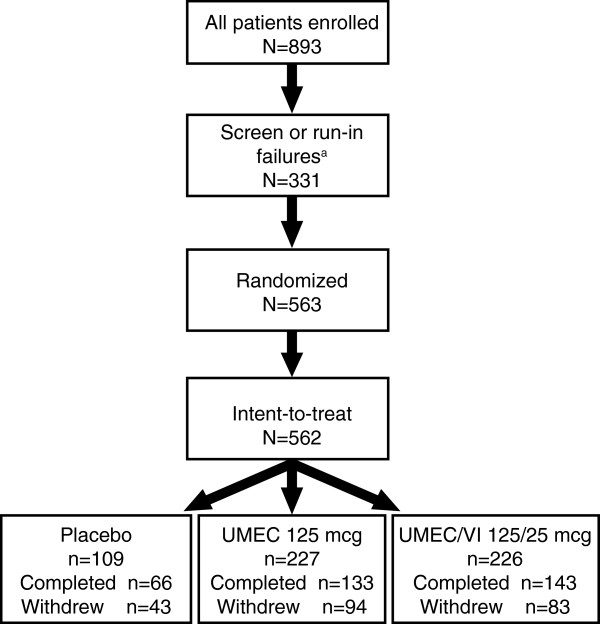
Methods: In this 52-week, double-blind, placebo-controlled, parallel-group safety study (GSK study DB2113359; NCT01316887), patients were randomized 2:2:1 to UMEC/VI 125/25 mcg, UMEC 125 mcg, or placebo. Study endpoints included adverse events (AEs), clinical chemistry and hematology parameters, vital signs, 12-lead, and 24-hour Holter electrocardiograms. COPD exacerbations and rescue medication use were assessed as safety parameters; lung function was also evaluated.
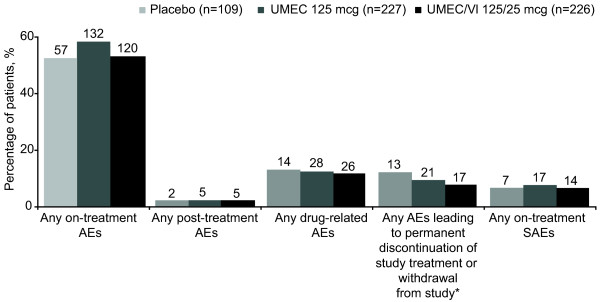
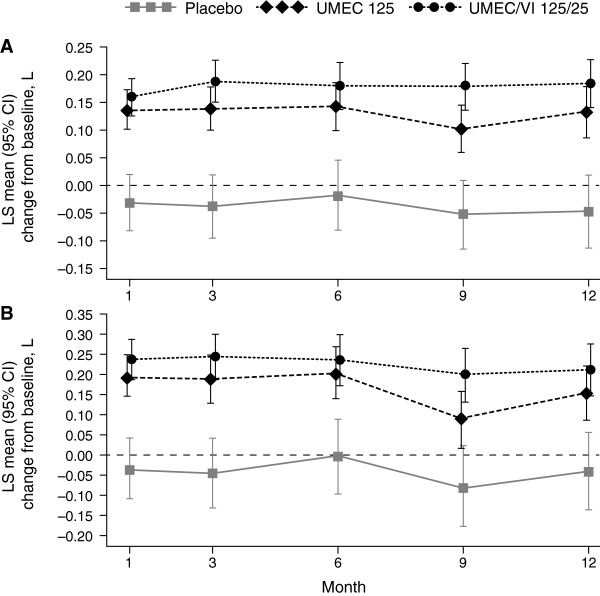
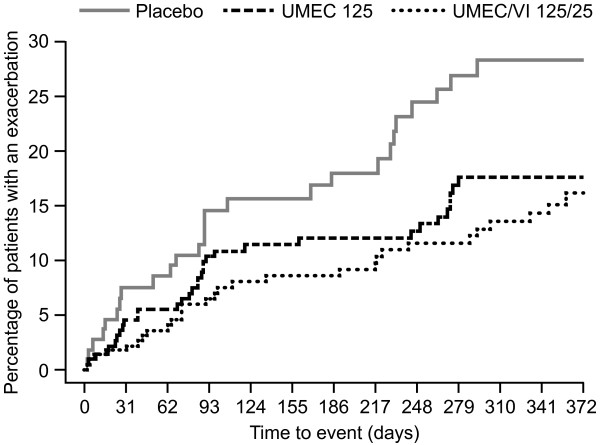
Results: The incidence of on-treatment AEs, serious AEs (SAEs), and drug-related AEs was similar between treatment groups (AEs: 52-58%; SAEs: 6-7%; drug-related AEs: 12-13%). Headache was the most common AE in each treatment group (8-11%). AEs associated with the LAMA and LABA pharmacologic classes occurred at a low incidence across treatment groups. No clinically meaningful effects on vital signs or laboratory assessments were reported for active treatments versus placebo. The incidences of atrial arrhythmias with UMEC/VI 125/25 mcg were similar to placebo; for UMEC 125 mcg, the incidences of ectopic supraventricular beats, sustained supraventricular tachycardia, and ectopic supraventricular rhythm were ≥2% greater than placebo. With active treatments, COPD exacerbations were fewer (13-15% of patients reporting ≥1 exacerbation) and on average less rescue medication was required (1.6-2.2 puffs/day) versus placebo (24% reporting ≥1 exacerbation, 2.6 puffs/day). Both active treatments improved lung function versus placebo.
Conclusion: UMEC/VI 125/25 mcg and UMEC 125 mcg were well tolerated over 12 months in patients with COPD.
Figures

References
-
- GOLD. Global strategy for the diagnosis, management and prevention of Chronic Obstructive Pulmonary Disease. 2014. [ http://www.goldcopd.org/uploads/users/files/GOLD_Report2014_Feb07.pdf]
-
- Brusasco V. Reducing cholinergic constriction: the major reversible mechanism in COPD. Eur Respir Rev. 2006;15:32–36. doi: 10.1183/09059180.00009902. - DOI
-
- Mahler DA, D’Urzo A, Bateman ED, Ozkan SA, White T, Peckitt C, Lassen C, Kramer B. INTRUST-1 and INTRUST-2 study investigators. Concurrent use of indacaterol plus tiotropium in patients with COPD provides superior bronchodilation compared with tiotropium alone: a randomised, double-blind comparison. Thorax. 2012;67:781–788. doi: 10.1136/thoraxjnl-2011-201140. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
