

Untreated brain arteriovenous malformation: patient-level meta-analysis of hemorrhage predictors
- PMID: 25015366
- PMCID: PMC4141996
- DOI: 10.1212/WNL.0000000000000688
Untreated brain arteriovenous malformation: patient-level meta-analysis of hemorrhage predictors
Abstract
Objective: To identify risk factors for intracranial hemorrhage in the natural history course of brain arteriovenous malformations (AVMs) using individual patient data meta-analysis of 4 existing cohorts.
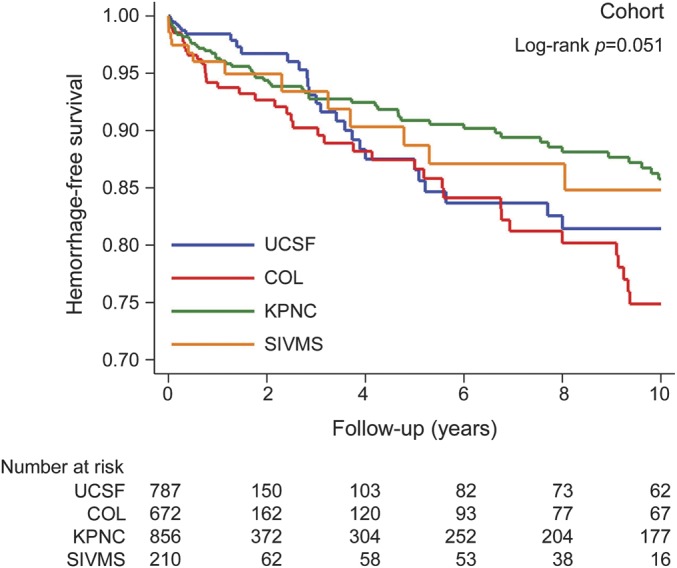
Methods: We harmonized data from Kaiser Permanente of Northern California (n = 856), University of California San Francisco (n = 787), Columbia University (n = 672), and the Scottish Intracranial Vascular Malformation Study (n = 210). We censored patients at first treatment, death, last visit, or 10-year follow-up, and performed stratified Cox regression analysis of time-to-hemorrhage after evaluating hemorrhagic presentation, sex, age at diagnosis, deep venous drainage, and AVM size as predictors. Multiple imputation was performed to assess impact of missing data.
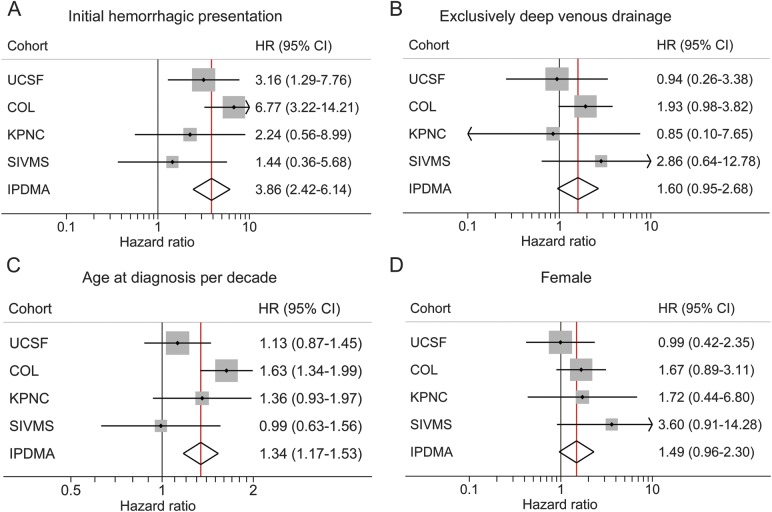
Results: A total of 141 hemorrhage events occurred during 6,074 patient-years of follow-up (annual rate of 2.3%, 95% confidence interval [CI] 2.0%-2.7%), higher for ruptured (4.8%, 3.9%-5.9%) than unruptured (1.3%, 1.0%-1.7%) AVMs at presentation. Hemorrhagic presentation (hazard ratio 3.86, 95% CI 2.42-6.14) and increasing age (1.34 per decade, 1.17-1.53) independently predicted hemorrhage and remained significant predictors in the imputed dataset. Female sex (1.49, 95% CI 0.96-2.30) and exclusively deep venous drainage (1.60, 0.95-2.68, p = 0.02 in imputed dataset) may be additional predictors. AVM size was not associated with intracerebral hemorrhage in multivariable models (p > 0.5).
Conclusion: This large, individual patient data meta-analysis identified hemorrhagic presentation and increasing age as independent predictors of hemorrhage during follow-up. Additional AVM cohort data may further improve precision of estimates, identify new risk factors, and allow validation of prediction models.
© 2014 American Academy of Neurology.
Figures
References
-
- Hernesniemi JA, Dashti R, Juvela S, Vaart K, Niemela M, Laakso A. Natural history of brain arteriovenous malformations: a long-term follow-up study of risk of hemorrhage in 238 patients. Neurosurgery 2008;63:823–831 - PubMed
-
- Halim AX, Johnston SC, Singh V, et al. Longitudinal risk of intracranial hemorrhage in patients with arteriovenous malformation of the brain within a defined population. Stroke 2004;35:1697–1702 - PubMed
-
- Wedderburn CJ, van Beijnum J, Bhattacharya JJ, et al. Outcome after interventional or conservative management of unruptured brain arteriovenous malformations: a prospective, population-based cohort study. Lancet Neurol 2008;7:223–230 - PubMed
-
- Kim H, Sidney S, McCulloch CE, et al. Racial/ethnic differences in longitudinal risk of intracranial hemorrhage in brain arteriovenous malformation patients. Stroke 2007;38:2430–2437 - PubMed
-
- da Costa L, Wallace MC, Ter Brugge KG, O'Kelly C, Willinsky RA, Tymianski M. The natural history and predictive features of hemorrhage from brain arteriovenous malformations. Stroke 2009;40:100–105 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources