

Role of gonadotropin-releasing hormone receptor mutations in patients with a wide spectrum of pubertal delay
- PMID: 25016926
- PMCID: PMC4149947
- DOI: 10.1016/j.fertnstert.2014.05.044
Role of gonadotropin-releasing hormone receptor mutations in patients with a wide spectrum of pubertal delay
Abstract
Objective: To analyze the GNRHR in patients with normosmic isolated hypogonadotropic hypogonadism (IHH) and constitutional delay of growth and puberty (CDGP).
Design: Molecular analysis and in vitro experiments correlated with phenotype.
Setting: Academic medical center.
Patient(s): A total of 110 individuals with normosmic IHH (74 male patients) and 50 with CDGP.
Intervention(s): GNRHR coding region was amplified and sequenced.
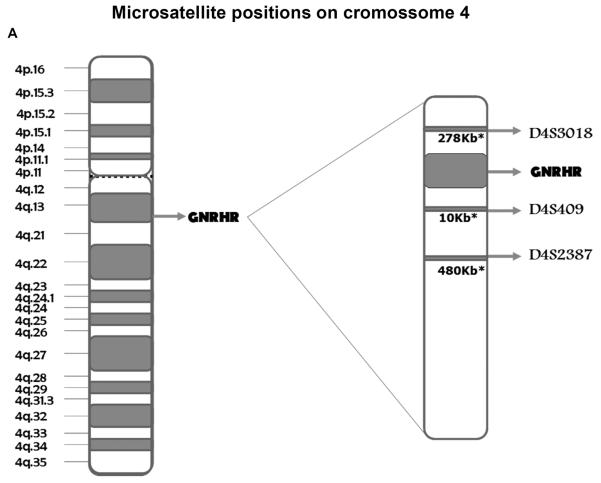
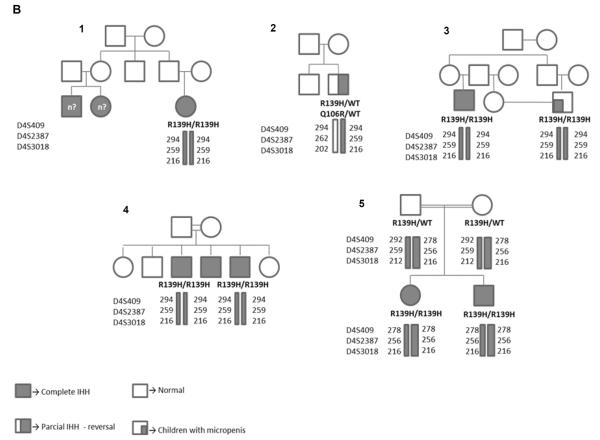
Main outcome measure(s): Novel variants were submitted to in vitro analysis. Frequency of mutations and genotype-phenotype correlation were analyzed. Microsatellite markers flanking GNRHR were examined in patients carrying the same mutation to investigate a possible founder effect.
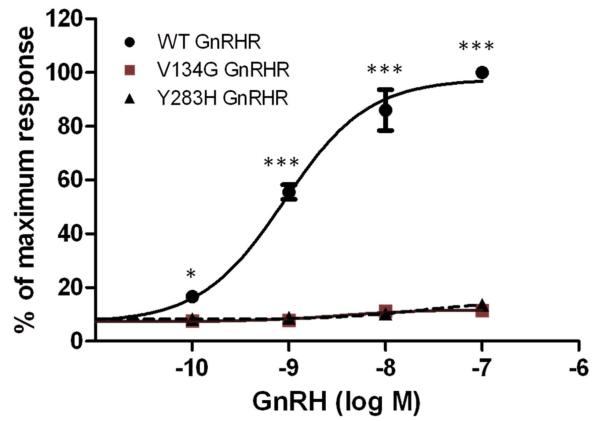
Result(s): Eleven IHH patients (10%) carried biallelic GNRHR mutations. In vitro analysis of novel variants (p.Y283H and p.V134G) demonstrated complete inactivation. The founder effect study revealed that Brazilian patients carrying the p.R139H mutation shared the same haplotype. Phenotypic spectrum in patients with GNRHR mutations varied from complete GnRH deficiency to partial and reversible IHH, with a relatively good genotype-phenotype correlation. One boy with CDGP was heterozygous for the p.Q106R variant, which was not considered to be pathogenic.
Conclusion(s): GNRHR mutations are a frequent cause of congenital normosmic IHH and should be the first candidate gene for genetic screening in this condition, especially in autosomal recessive familial cases. The founder effect study suggested that the p.R139H mutation arises from a common ancestor in the Brazilian population. Finally, mutations in GNRHR do not appear to be involved in the pathogenesis of CDGP.
Keywords: GnRH receptor; founder effect; hypogonadotropic hypogonadism; mutation; pubertal delay.
Copyright © 2014 American Society for Reproductive Medicine. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Palmert MR, Boepple PA. Variation in the timing of puberty: clinical spectrum and genetic investigation. J Clin Endocrinol Metab. 2001;86(6):2364–8. - PubMed
-
- Palmert MR, Dunkel L. Clinical practice. Delayed puberty. N Engl J Med. 2012;366(5):443–53. Epub 2012/02/03. - PubMed
-
- Seminara SB, Hayes FJ, Crowley WF., Jr. Gonadotropin-releasing hormone deficiency in the human (idiopathic hypogonadotropic hypogonadism and Kallmann's syndrome): pathophysiological and genetic considerations. Endocr Rev. 1998;19(5):521–39. - PubMed
-
- Quinton R, Duke VM, Robertson A, Kirk JM, Matfin G, de Zoysa PA, et al. Idiopathic gonadotrophin deficiency: genetic questions addressed through phenotypic characterization. Clin Endocrinol (Oxf) 2001;55(2):163–74. - PubMed
-
- de Roux N, Young J, Misrahi M, Genet R, Chanson P, Schaison G, et al. A family with hypogonadotropic hypogonadism and mutations in the gonadotropin-releasing hormone receptor. N Engl J Med. 1997;337(22):1597–602. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
