

Children's Hospital Association consensus statements for comorbidities of childhood obesity
- PMID: 25019404
- PMCID: PMC4120655
- DOI: 10.1089/chi.2013.0120
Children's Hospital Association consensus statements for comorbidities of childhood obesity
Abstract
Background: Childhood obesity and overweight affect approximately 30% of US children. Many of these children have obesity-related comorbidities, such as hypertension, dyslipidemia, fatty liver disease, diabetes, polycystic ovary syndrome (PCOS), sleep apnea, psychosocial problems, and others. These children need routine screening and, in many cases, treatment for these conditions. However, because primary care pediatric providers (PCPs) often are underequipped to deal with these comorbidities, they frequently refer these patients to subspecialists. However, as a result of the US pediatric subspecialist shortage and considering that 12.5 million children are obese, access to care by subspecialists is limited. The aim of this article is to provide accessible, user-friendly clinical consensus statements to facilitate the screening, interpretation of results, and early treatment for some of the most common childhood obesity comorbidities.
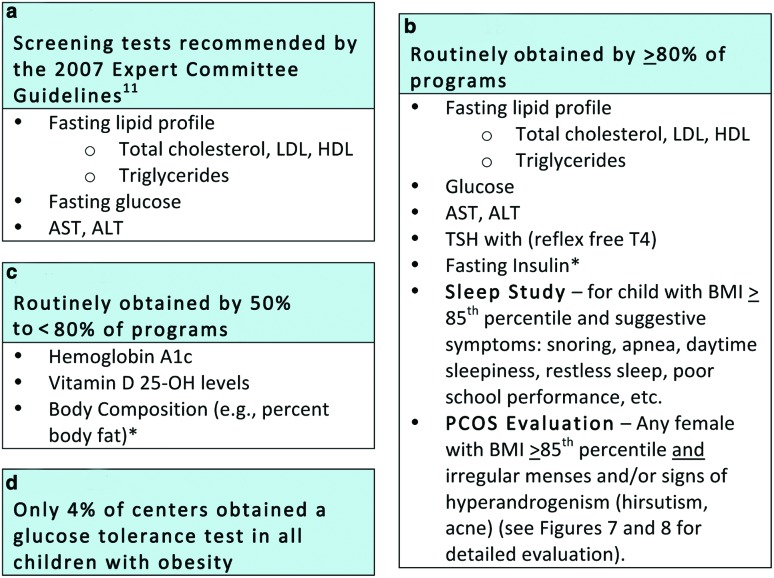
Methods: Members of the Children's Hospital Association (formerly NACHRI) FOCUS on a Fitter Future II (FFFII), a collaboration of 25 US pediatric obesity centers, used a combination of the best available evidence and collective clinical experience to develop consensus statements for pediatric obesity-related comorbidities. FFFII also surveyed the participating pediatric obesity centers regarding their current practices.
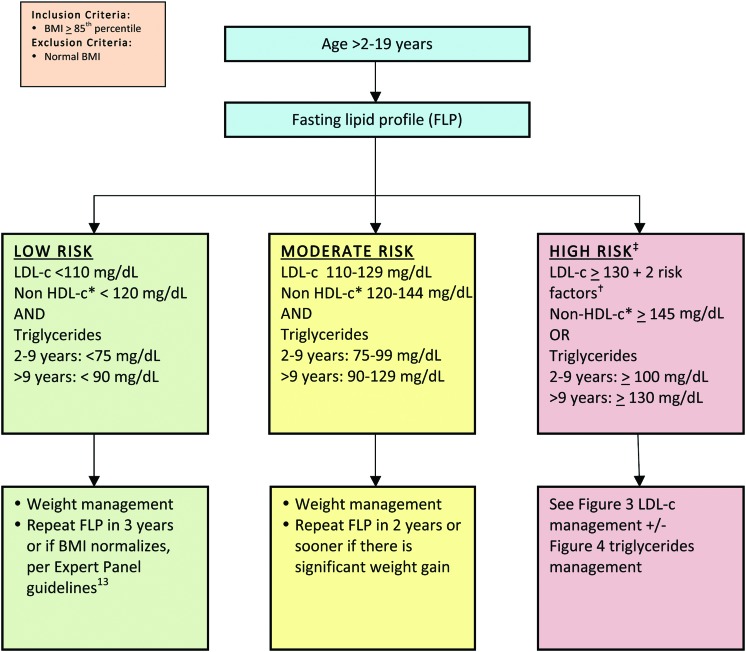
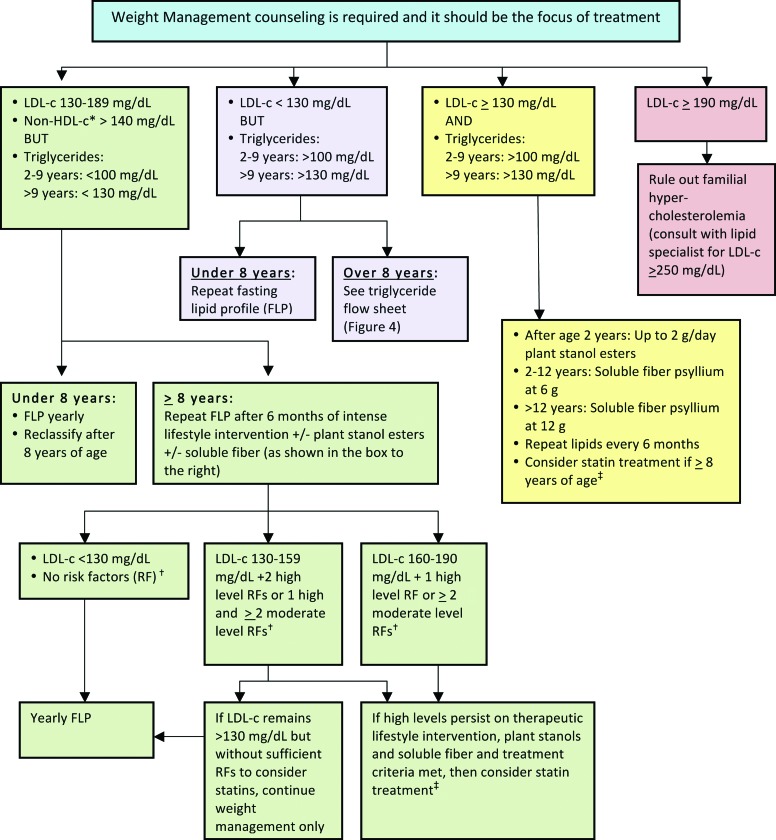
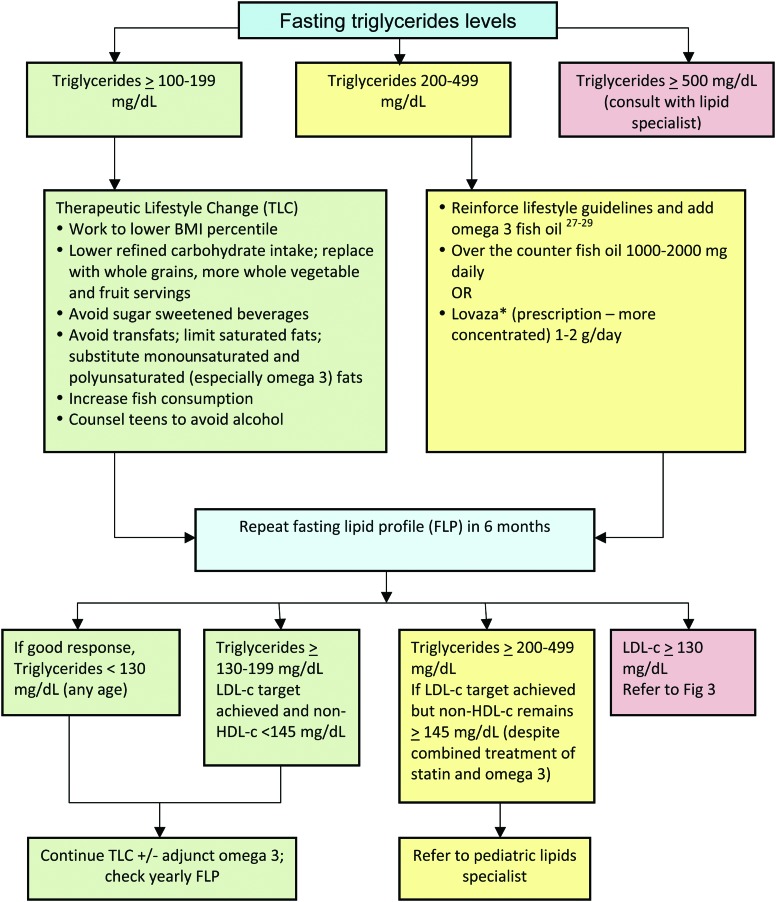
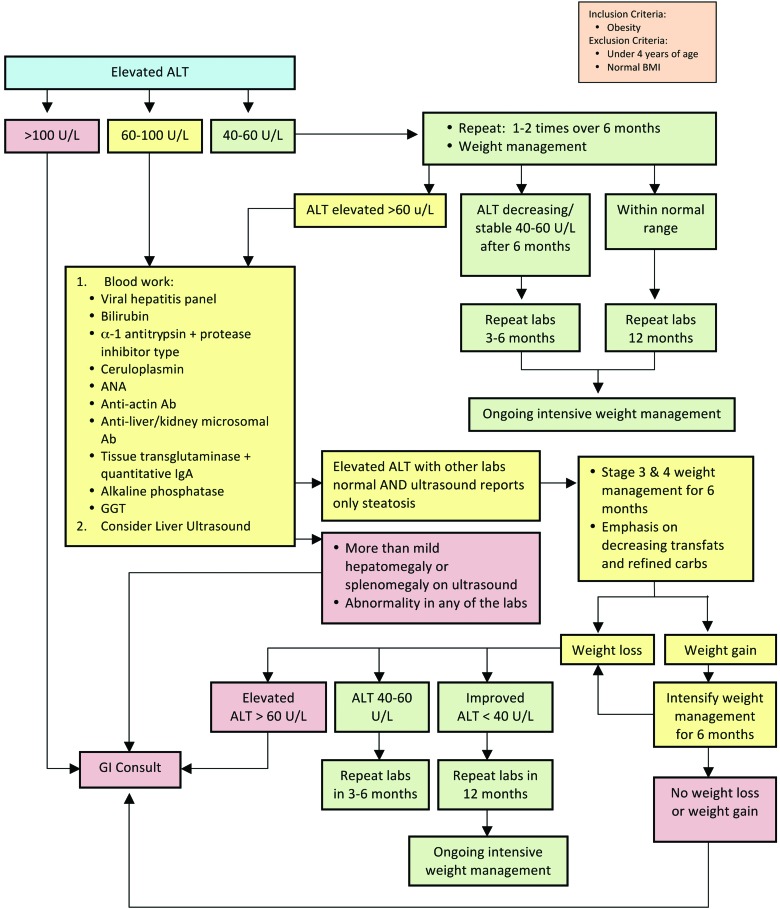
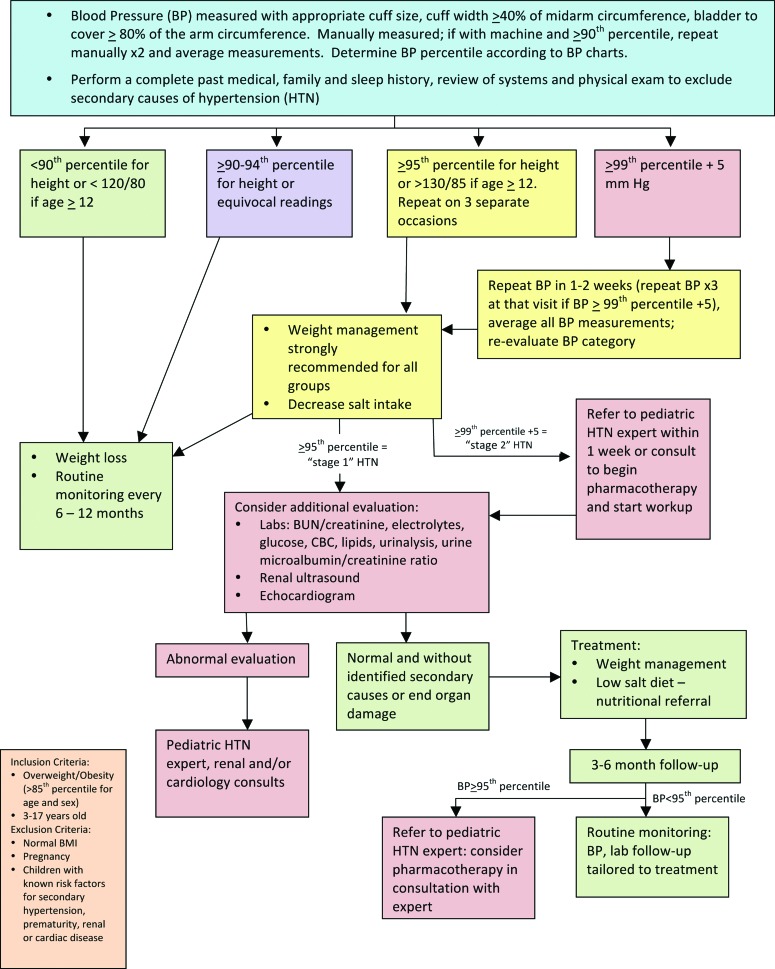
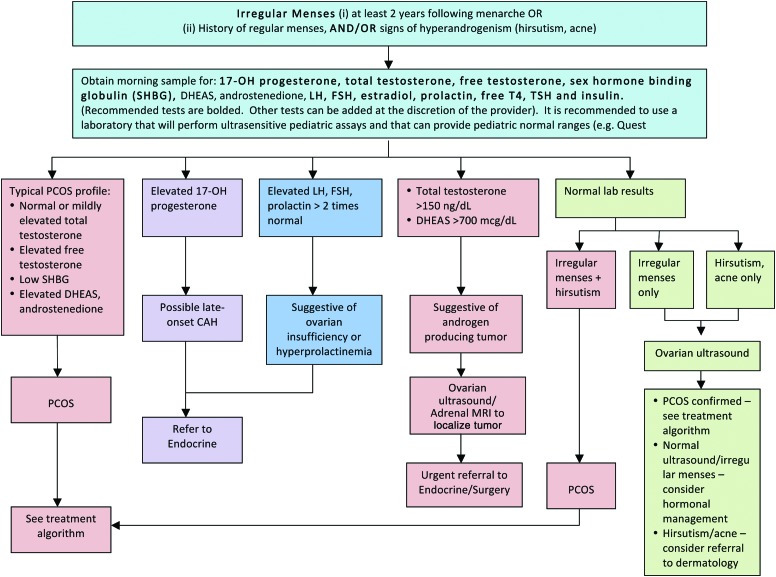
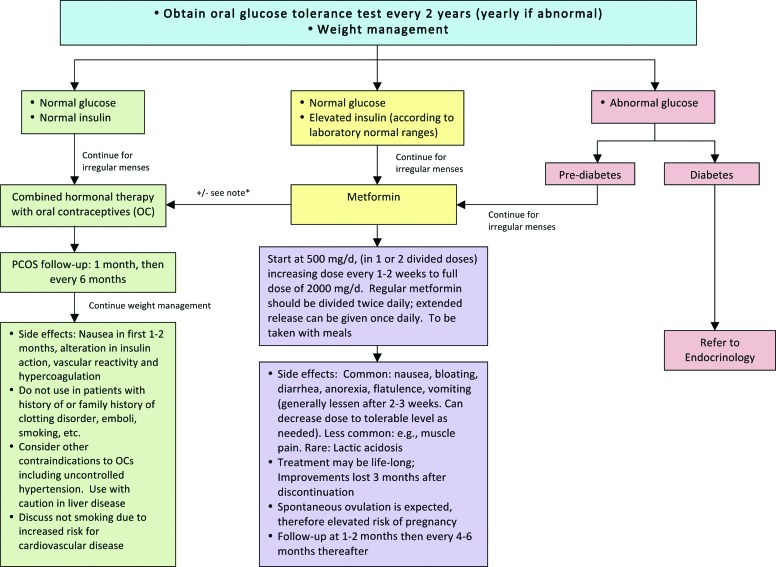
Results: The work group developed consensus statements for use in the evaluation and treatment of lipids, liver enzymes, and blood pressure abnormalities and PCOS in the child with overweight and obesity. The results of the FFFII survey illustrated the variability in the approach for initial evaluation and treatment as well as pattern of referrals to subspecialists among programs.
Conclusions: The consensus statements presented in this article can be a useful tool for PCPs in the management and overall care of children with overweight and obesity.
Figures
Comment in
-
Re: Estrada et al., "Children's Hospital Association Consensus Statements for Comorbidities of Childhood Obesity".Child Obes. 2015 Jun;11(3):231-2. doi: 10.1089/chi.2015.0035. Child Obes. 2015. PMID: 26034812 No abstract available.
References
-
- Odgen C, Carroll M. Prevalence of obesity among children and adolescents: United States, trends 1963–1965 through 2007–2008. CDC, National Center for Health Statistics: Atlanta, GA, 2010
-
- Rubin CM. Management of pediatric overweight/obesity: A survey of primary care providers. Is it time for a clinical alternative? Child Obes 2011;7:400–408
-
- Zamosky L. The obesity epidemic. While America swallows $147 billion in obesity-related healthcare costs, physicians called on to confront the crisis. Med Econ 2013;90:14–17 - PubMed
-
- Mazur A, Matusik P, Revert K, et al. Childhood obesity: Knowledge, attitudes, and practices of European pediatric care providers. Pediatrics 2013;132:e100–e108 - PubMed
-
- Walsh CO, Milliren CE, Feldman HA, et al. Factors affecting subspecialty referrals by pediatric primary care providers for children with obesity-related comorbidities. Clin Pediatr (Phila) 2013;52:777–785 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
