

Optimization of MR imaging for pretreatment evaluation of patients with endometrial and cervical cancer
- PMID: 25019443
- PMCID: PMC4307629
- DOI: 10.1148/rg.344140001
Optimization of MR imaging for pretreatment evaluation of patients with endometrial and cervical cancer
Abstract
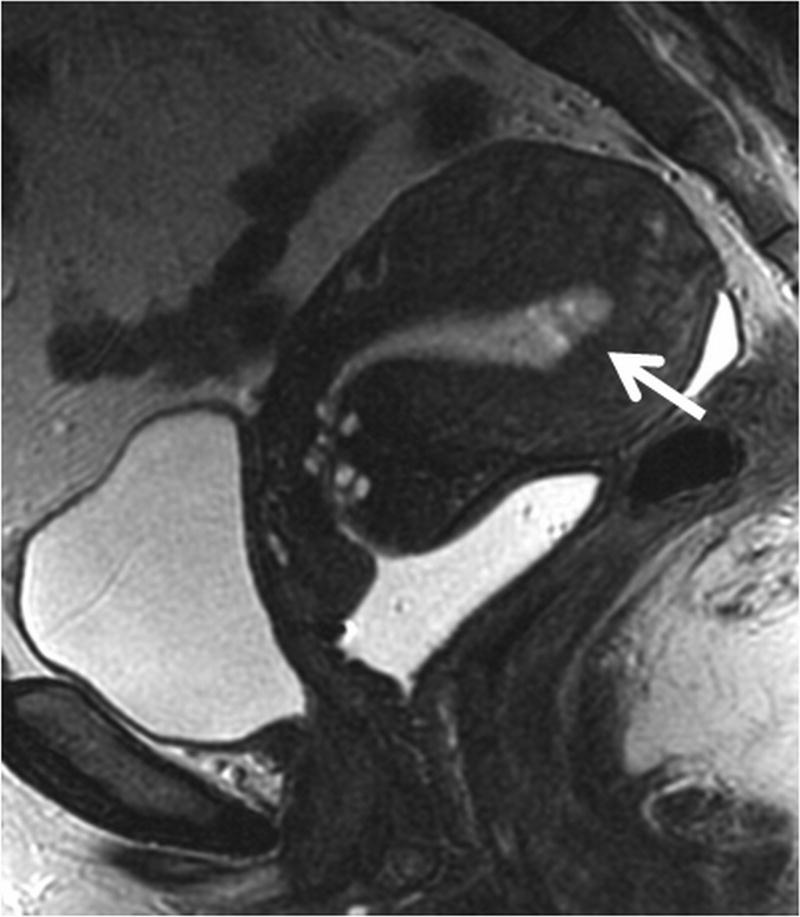
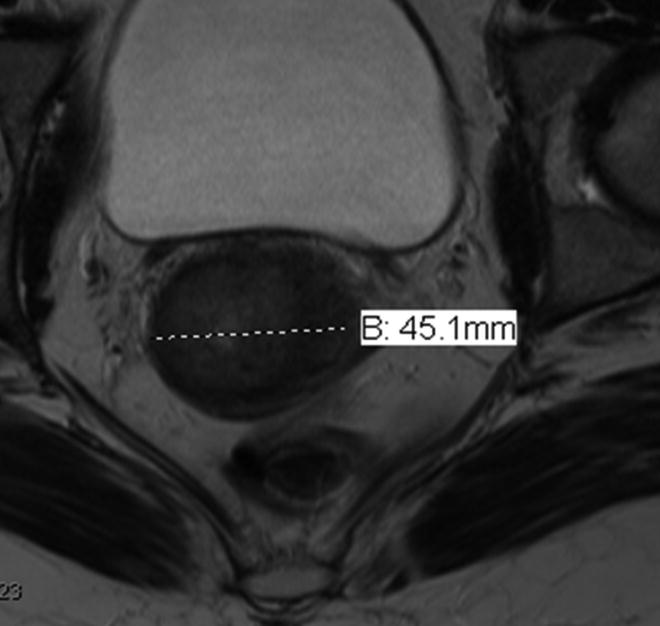
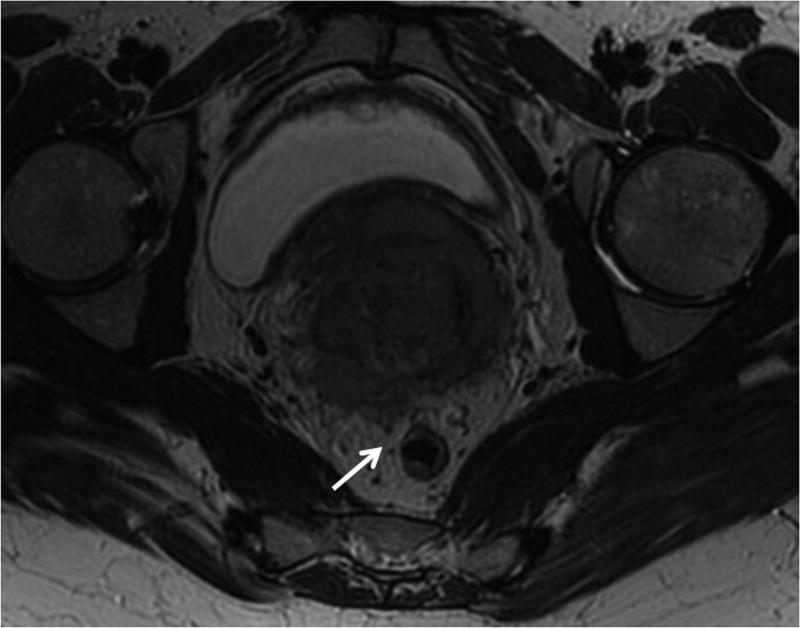
Endometrial and cervical cancer are the most common gynecologic malignancies in the world. Accurate staging of cervical and endometrial cancer is essential to determine the correct treatment approach. The current International Federation of Gynecology and Obstetrics (FIGO) staging system does not include modern imaging modalities. However, magnetic resonance (MR) imaging has proved to be the most accurate noninvasive modality for staging endometrial and cervical carcinomas and often helps with risk stratification and making treatment decisions. Multiparametric MR imaging is increasingly being used to evaluate the female pelvis, an approach that combines anatomic T2-weighted imaging with functional imaging (ie, dynamic contrast material-enhanced and diffusion-weighted imaging). MR imaging helps guide treatment decisions by depicting the depth of myometrial invasion and cervical stromal involvement in patients with endometrial cancer and tumor size and parametrial invasion in those with cervical cancer. However, its accuracy for local staging depends on technique and image quality, namely thin-section high-resolution multiplanar T2-weighted imaging with simple modifications, such as double oblique T2-weighting supplemented by diffusion weighting and contrast enhancement.
©RSNA, 2014.
Figures



































References
-
- Howlader N, Noone A, Krapcho M, et al. SEER Cancer Statistics Review (CSR), 1975–2010. [Accessed April 8, 2013];National Cancer Institute [serial online] 2012 Available at: http://seer.cancer.gov/csr/1975_2010/
-
- Sala E, Wakely S, Senior E, Lomas D. MRI of malignant neoplasms of the uterine corpus and cervix. AJR Am J Roentgenol. 2007;188(6):1577–1587. - PubMed
-
- Lewin SN. Revised FIGO staging system for endometrial cancer. Clin Obstet Gynecol. 2011;54(2):215–218. - PubMed
-
- Sala E, Rockall A, Kubik-Huch RA. Advances in magnetic resonance imaging of endometrial cancer. Eur Radiol. 2011;21(3):468–473. - PubMed
-
- Larson DM, Connor GP, Broste SK, Krawisz BR, Johnson KK. Prognostic significance of gross myometrial invasion with endometrial cancer. Obstet Gynecol. 1996;88(3):394–398. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
