

At the interface of sensory and motor dysfunctions and Alzheimer's disease
- PMID: 25022540
- PMCID: PMC4287457
- DOI: 10.1016/j.jalz.2014.04.514
At the interface of sensory and motor dysfunctions and Alzheimer's disease
Abstract
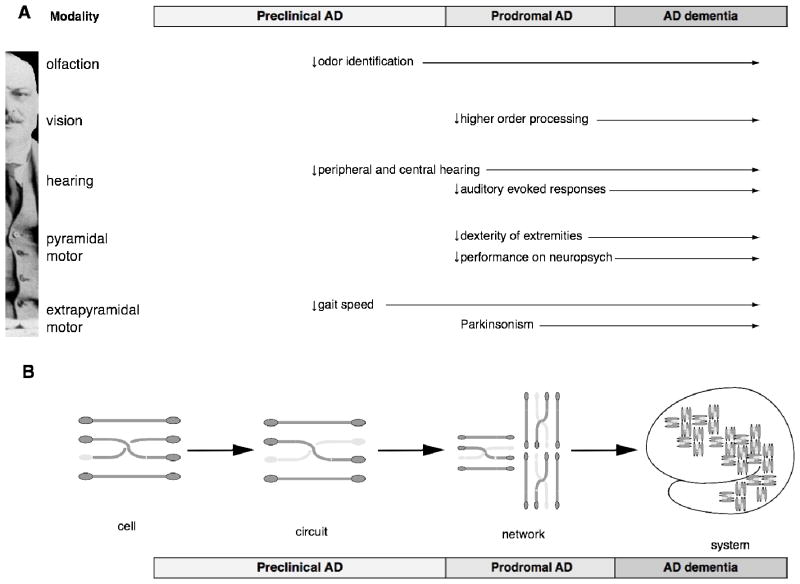
Recent evidence indicates that sensory and motor changes may precede the cognitive symptoms of Alzheimer's disease (AD) by several years and may signify increased risk of developing AD. Traditionally, sensory and motor dysfunctions in aging and AD have been studied separately. To ascertain the evidence supporting the relationship between age-related changes in sensory and motor systems and the development of AD and to facilitate communication between several disciplines, the National Institute on Aging held an exploratory workshop titled "Sensory and Motor Dysfunctions in Aging and AD." The scientific sessions of the workshop focused on age-related and neuropathologic changes in the olfactory, visual, auditory, and motor systems, followed by extensive discussion and hypothesis generation related to the possible links among sensory, cognitive, and motor domains in aging and AD. Based on the data presented and discussed at this workshop, it is clear that sensory and motor regions of the central nervous system are affected by AD pathology and that interventions targeting amelioration of sensory-motor deficits in AD may enhance patient function as AD progresses.
Keywords: Aging; Alzheimer's disease; Auditory function; Motor; Olfaction; Sensory; Vision.
Copyright © 2015 The Alzheimer's Association. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Wilson RS, Schneider JA, Bienias JL, Evans DA, Bennett DA. Parkinsonianlike signs and risk of incident Alzheimer disease in older persons. Arch Neurol. 2003;60(4):539–44. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 AG044920/AG/NIA NIH HHS/United States
- P30 AG010124/AG/NIA NIH HHS/United States
- RF1 AG015819/AG/NIA NIH HHS/United States
- P50 AG005146/AG/NIA NIH HHS/United States
- R01 AG041795/AG/NIA NIH HHS/United States
- R01 AG017917/AG/NIA NIH HHS/United States
- K23 DC011279/DC/NIDCD NIH HHS/United States
- R01 AG015819/AG/NIA NIH HHS/United States
- R01 AG019714/AG/NIA NIH HHS/United States
- R01 AG031278/AG/NIA NIH HHS/United States
- P30 AG062421/AG/NIA NIH HHS/United States
- R01 AG038791/AG/NIA NIH HHS/United States
- DP2 OD006662/OD/NIH HHS/United States
- R01 DC008983/DC/NIDCD NIH HHS/United States
- R01 AG004085/AG/NIA NIH HHS/United States
- P50 AG005134/AG/NIA NIH HHS/United States
- P30 AG008017/AG/NIA NIH HHS/United States
- R21 NS085711/NS/NINDS NIH HHS/United States
- R01 AG037693/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
