

Delivering evidence-based smoking cessation treatment in primary care practice: experience of Ontario family health teams
- PMID: 25022655
- PMCID: PMC4096282
Delivering evidence-based smoking cessation treatment in primary care practice: experience of Ontario family health teams
Abstract
Objective: To report on the delivery of evidence-based smoking cessation treatments (EBSCTs) within a sample of 40 Ontario family health teams (FHTs).
Design: In each FHT, consecutive patients were screened for smoking status and eligible patients completed a questionnaire immediately following their clinic visits (index visits). Multilevel analysis was used to examine FHT-level, provider-level, and patient-level predictors of EBSCT delivery.
Setting: Forty FHTs in Ontario.
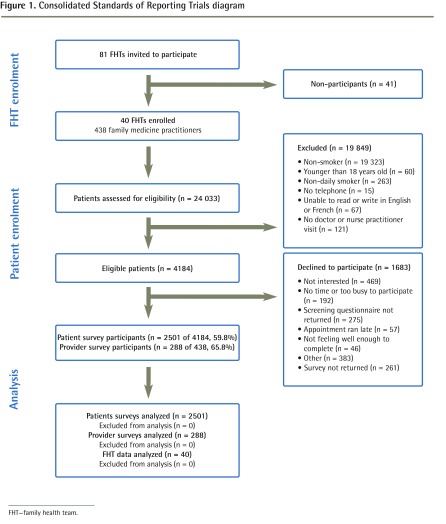
Participants: Across the 40 participating FHTs, 24,033 patients were screened and 2501 eligible patients contributed data.
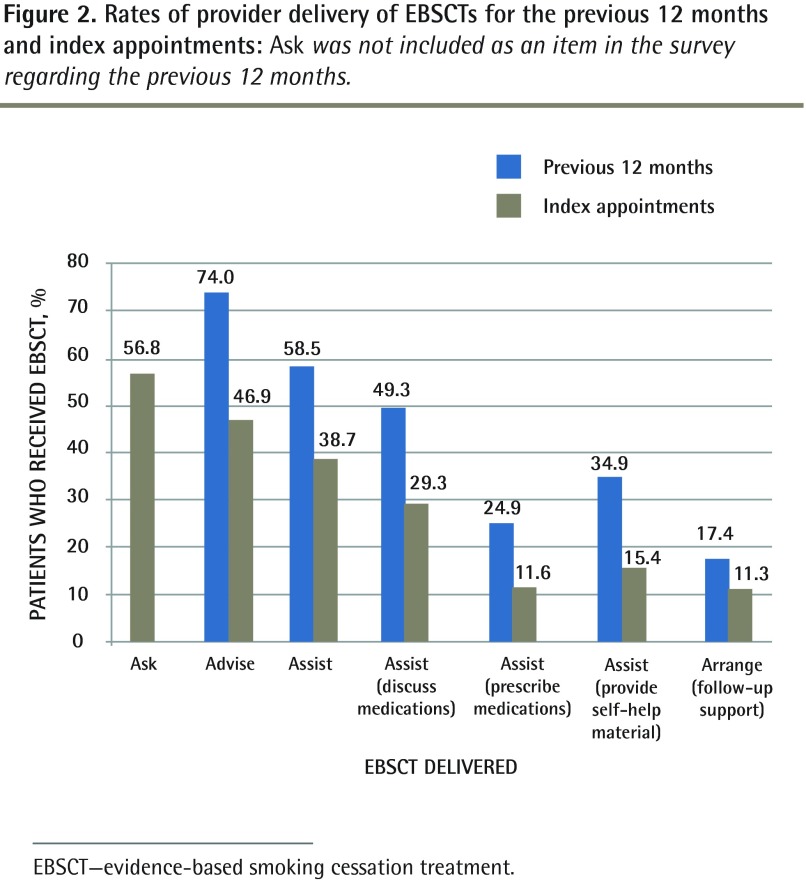
Main outcome measures: Provider performance in the delivery of EBSCTs during the preceding 12 months and during the index visits was assessed.
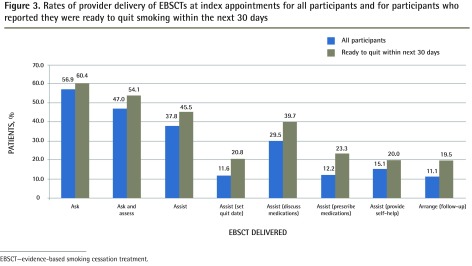
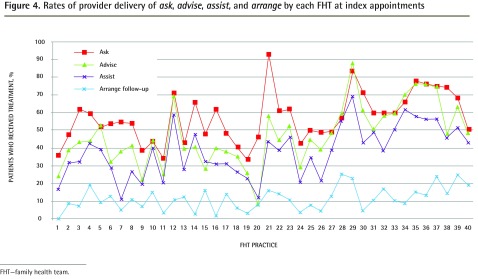
Results: The rate of provider delivery of EBSCT for the previous 12 months was 74.0% for the advise strategy. At the index visit, rates of EBSCT strategy delivery were 56.8% for ask; 46.9% for advise; 38.7% for assist; 11.6% for prescribing pharmacotherapy; and 11.3% for arrange follow-up. Significant intra-FHT and intraprovider variability in the rates of EBSCT delivery was identified. Family health teams with a physician champion (odds ratio [OR] 2.0; 95% CI 1.1 to 3.6; P < .01) and providers who highly ranked the importance of smoking cessation (OR 1.7; 95% CI 1.1 to 2.7; P < .01) were more likely to deliver EBSCTs. Patient readiness to quit (OR 1.6; 95% CI 1.3 to 1.9; P < .001), presence of smoking-related illness (OR 1.6; 95% CI 1.2 to 2.1; P < .01), and presenting for an annual health examination (OR 2.0; 95% CI 1.6 to 2.5; P < .001) were associated with the delivery of EBSCTs.
Conclusion: Rates of smoking cessation advice were higher than previously reported for Canadian physicians; however, rates of assistance with quitting were lower. Future quality improvement initiatives should specifically target increasing the rates of screening and advising among low-performing FHTs and providers within FHTs, with a particular emphasis on doing so at all clinic appointments; and improving the rate at which assistance with quitting is delivered.
Objectif: Décrire comment 40 équipes de santé familiale (ÉMF) de l’Ontario ont offert un traitement fondé sur des preuves visant l’arrêt du tabagisme (TFPAT).
Type d‘étude: Dans chaque ÉMF, on a questionné des patients consécutifs pour établir leur statut de fumeur; les patients éligibles ont répondu à un questionnaire immédiatement après leur visite à la clinique (visite repère). Une analyse multiniveau a été utilisée pour établir les prédicteurs de l’utilisation du TFPAT dans le cas des ÉMF, des soignants et des patients.
Contexte: Quatre ÉMF de l’Ontario.
Participants: Pour l’ensemble des 40 ÉMF participantes, 24 033 patients ont été questionnés; les données utilisées proviennent des 2 501 patients éligibles.
Principaux paramètres à l’étude: On a vérifié l’utilisation du TFPAT au cours des 12 mois précédant la visite repère ainsi que durant cette visite.
Résultats: Au cours des 12 mois précédant la visite repère, le taux d’utilisation du TFPAT était de 74,0 % dans le cas de la stratégie «conseiller». À la visite indice, le taux d’utilisation des stratégies du TFPAT était 56,8 % pour «s’informer»; 46,9 % pour «conseiller»; 38,7 % pour «assister»; 11,6 % pour «prescrire» une médication; et 11,3 % pour «planifier un suivi. Il y avait des différences significatives entre les ÉMF et entre les soignants pour ce qui est du taux d’utilisation du TFPAT. Les équipes de médecine familiale les plus susceptibles d’utiliser le TFPAT étaient celles qui comprenaient un médecin «champion» (rapport de cotes [RC] 2,0; IC à 95 % 1,1 à 3,6; P < ,01) ou celles où les soignants attribuaient une grande importance à l’arrêt du tabac (RC 1,7; IC à 95 % 1,1 à 2,7; P < ,01). On notait une association entre l’utilisation du TFPAT et le fait pour le patient d’avoir l’intention d’arrêter (RC 1,6; IC à 95 % 1,3 à 1,9; P < ,001), d’avoir une maladie liée au tabagisme (RC 1,6; IC à 95 % 1,2 à 2,1; P < ,01) et de se présenter pour un bilan de santé annuel (RC 2,0; IC à 95 % 1,6 à 2,5; P < ,001).
Conclusion: Le taux du recours à des conseils incitant à cesser de fumer était plus haut que celui antérieurement rapporté pour les médecins canadiens; toutefois, le taux d’assistance à cesser de fumer était plus bas. Les stratégies futures pour améliorer la qualité devraient chercher à obtenir de meilleurs taux de dépistage et de conseils parmi les ÉMF et les soignants des ÉMF peu performants, en insistant sur le fait de le faire à tous les rendez-vous, tout en visant une amélioration du taux d’utilisation de l’assistance à cesser de fumer.
Copyright© the College of Family Physicians of Canada.
Figures
References
-
- Ministry of Health and Long-Term Care. We’re making progress. FHT to Print. 2011 Summer-Fall; Available from: www.health.gov.on.ca/en/pro/programs/fht/docs/fht_news_201110.pdf. Accessed 2014 Jun 19.
-
- Ministry of Health and Long Term Care. Guide to communications. Toronto, ON: Ministry of Health and Long-Term Care; 2006. Available from: www.health.gov.on.ca/en/pro/programs/fht/docs/fht_communications2.pdf. Accessed 2014 Jun 25.
-
- Reid JL, Hammond D, Burkhalter R, Rynard VL, Ahmed R. Tobacco use in Canada: patterns and trends. 2013 ed. Waterloo, ON: Propel Centre for Population Health, University of Waterloo; 2013.
-
- Rehm J, Baliunas D, Brochu S, Fischer B, Gnam W, Patra J, et al. The costs of substance abuse in Canada 2002. Highlights. Ottawa, ON: Canadian Centre on Substance Abuse; 2006.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical