

Personalizing age of cancer screening cessation based on comorbid conditions: model estimates of harms and benefits
- PMID: 25023249
- PMCID: PMC4160041
- DOI: 10.7326/M13-2867
Personalizing age of cancer screening cessation based on comorbid conditions: model estimates of harms and benefits
Abstract
Background: Harms and benefits of cancer screening depend on age and comorbid conditions, but reliable estimates are lacking.
Objective: To estimate the harms and benefits of cancer screening by age and comorbid conditions to inform decisions about screening cessation.
Design: Collaborative modeling with 7 cancer simulation models and common data on average and comorbid condition level-specific life expectancy.
Setting: U.S. population.
Patients: U.S. cohorts aged 66 to 90 years in 2010 with average health or 1 of 4 comorbid condition levels: none, mild, moderate, or severe.
Intervention: Mammography, prostate-specific antigen testing, or fecal immunochemical testing.
Measurements: Lifetime cancer deaths prevented and life-years gained (benefits); false-positive test results and overdiagnosed cancer cases (harms). For each comorbid condition level, the age at which harms and benefits of screening were similar to that for persons with average health having screening at age 74 years.
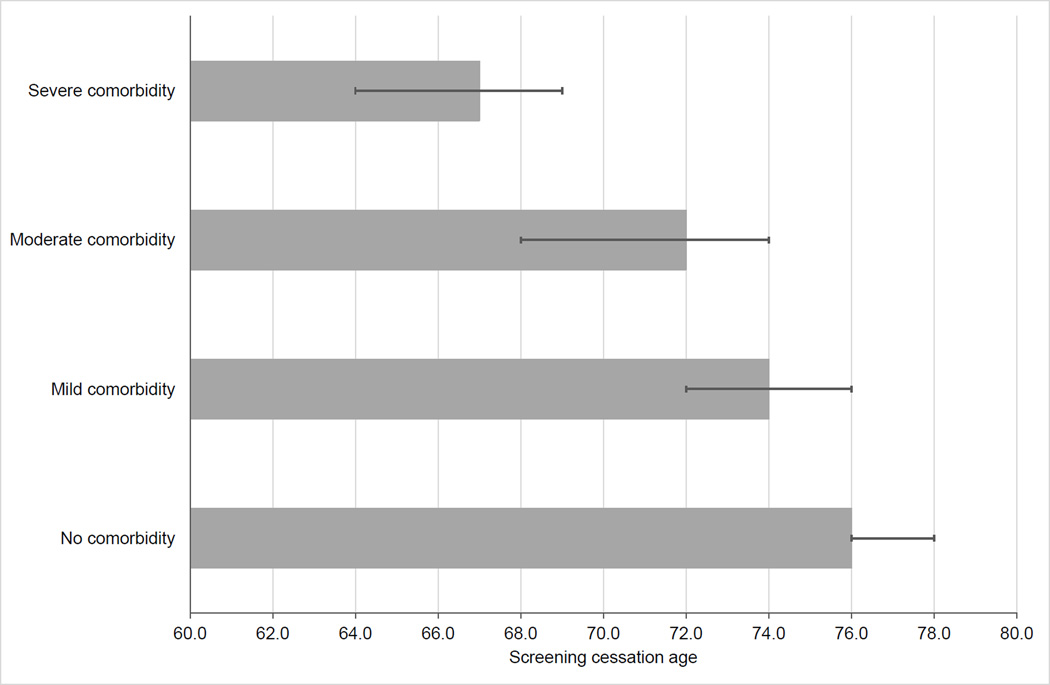
Results: Screening 1000 women with average life expectancy at age 74 years for breast cancer resulted in 79 to 96 (range across models) false-positive results, 0.5 to 0.8 overdiagnosed cancer cases, and 0.7 to 0.9 prevented cancer deaths. Although absolute numbers of harms and benefits differed across cancer sites, the ages at which to cease screening were consistent across models and cancer sites. For persons with no, mild, moderate, and severe comorbid conditions, screening until ages 76, 74, 72, and 66 years, respectively, resulted in harms and benefits similar to average-health persons.
Limitation: Comorbid conditions influenced only life expectancy.
Conclusion: Comorbid conditions are an important determinant of harms and benefits of screening. Estimates of screening benefits and harms by comorbid condition can inform discussions between providers and patients about personalizing screening cessation decisions.
Primary funding source: National Cancer Institute and Centers for Disease Control and Prevention.
Figures

Summary for patients in
-
Summaries for patients. Personalizing age of cancer screening cessation.Ann Intern Med. 2014 Jul 15;161(2). doi: 10.7326/P14-9023. Ann Intern Med. 2014. PMID: 25023262 No abstract available.
References
-
- U. S. Preventive Services Task Force. Screening for colorectal cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2008 Nov 4;149(9):627–637. - PubMed
-
- U. S. Preventive Services Task Force. Screening for breast cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2009 Nov 17;151(10):716–726. W-236. - PubMed
-
- Smith RA, Cokkinides V, Brawley OW. Cancer screening in the United States, 2012: A review of current American Cancer Society guidelines and current issues in cancer screening. CA Cancer J Clin. 2012;62:129–142. - PubMed
-
- 2012 National Population Projections: Table 1. Projected Population by Single Year of Age, Sex, Race, and Hispanic Origin for the United States: 2012 to 2060 [database on the Internet]. U.S. Census Bureau, Population Division. 2012. [on March 17, 2013]; Accessed at http://www.census.gov/population/projections/data/national/2012/download....
Publication types
MeSH terms
Substances
Grants and funding
- U01 CA152958/CA/NCI NIH HHS/United States
- U01 CA063740/CA/NCI NIH HHS/United States
- U01CA152959/CA/NCI NIH HHS/United States
- U01 CA115953/CA/NCI NIH HHS/United States
- U01 CA097426/CA/NCI NIH HHS/United States
- U01 CA086082/CA/NCI NIH HHS/United States
- P01 CA154292/CA/NCI NIH HHS/United States
- P01CA154292/CA/NCI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- U01CA152958/CA/NCI NIH HHS/United States
- UM1 CA182883/CA/NCI NIH HHS/United States
- U01 CA152959/CA/NCI NIH HHS/United States
- U01 CA070040/CA/NCI NIH HHS/United States
- U01CA088283/CA/NCI NIH HHS/United States
- U01CA115953/CA/NCI NIH HHS/United States
- U01 CA063731/CA/NCI NIH HHS/United States
- U01 CA086076/CA/NCI NIH HHS/United States
- U01 CA069976/CA/NCI NIH HHS/United States
- U01 CA063736/CA/NCI NIH HHS/United States
- K05 CA096940/CA/NCI NIH HHS/United States
- U01CA157224/CA/NCI NIH HHS/United States
- U01CA097426/CA/NCI NIH HHS/United States
- U01 CA070013/CA/NCI NIH HHS/United States
- K05CA96940/CA/NCI NIH HHS/United States
- U01 CA088283/CA/NCI NIH HHS/United States
- U01 CA157224/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous