

Pediatric cancer type predicts infection rate, need for critical care intervention, and mortality in the pediatric intensive care unit
- PMID: 25023526
- PMCID: PMC4177269
- DOI: 10.1007/s00134-014-3389-2
Pediatric cancer type predicts infection rate, need for critical care intervention, and mortality in the pediatric intensive care unit
Abstract
Purpose: Up to 38 % of children with cancer require pediatric intensive care unit (PICU) admission within 3 years of diagnosis, with reported PICU mortality of 13-27 % far exceeding that of the general PICU population. PICU outcomes data for individual cancer types are lacking and may help identify patients at risk for poor clinical outcomes.
Methods: We performed a retrospective multicenter analysis of 10,365 PICU admissions of cancer patients no greater than 21 years old among 112 PICUs between 1 January 2009 and 30 June 2012. We evaluated the effect of cancer type, age, gender, genetic syndrome, stem cell transplantation, PRISM3 score, infections, and critical care interventions on PICU mortality.
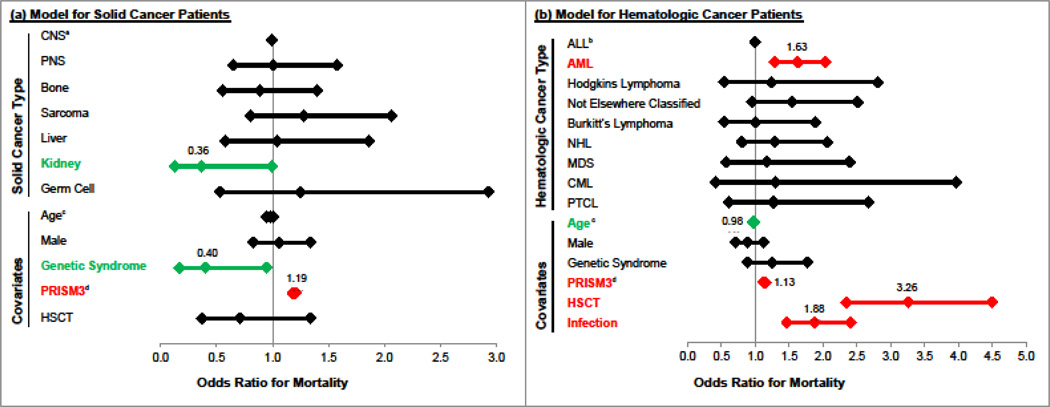
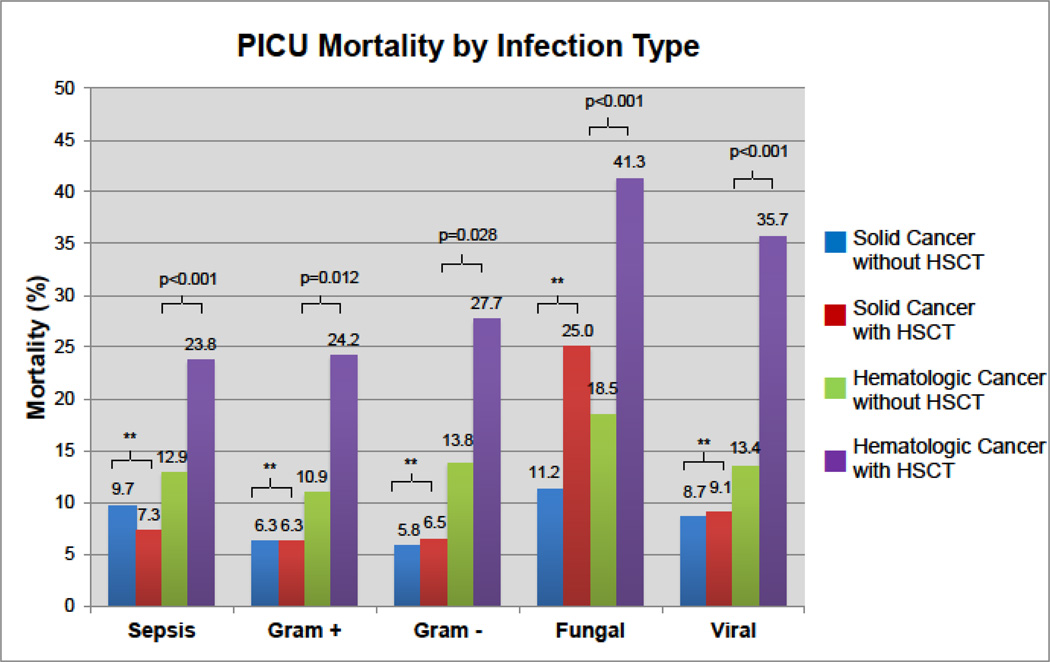
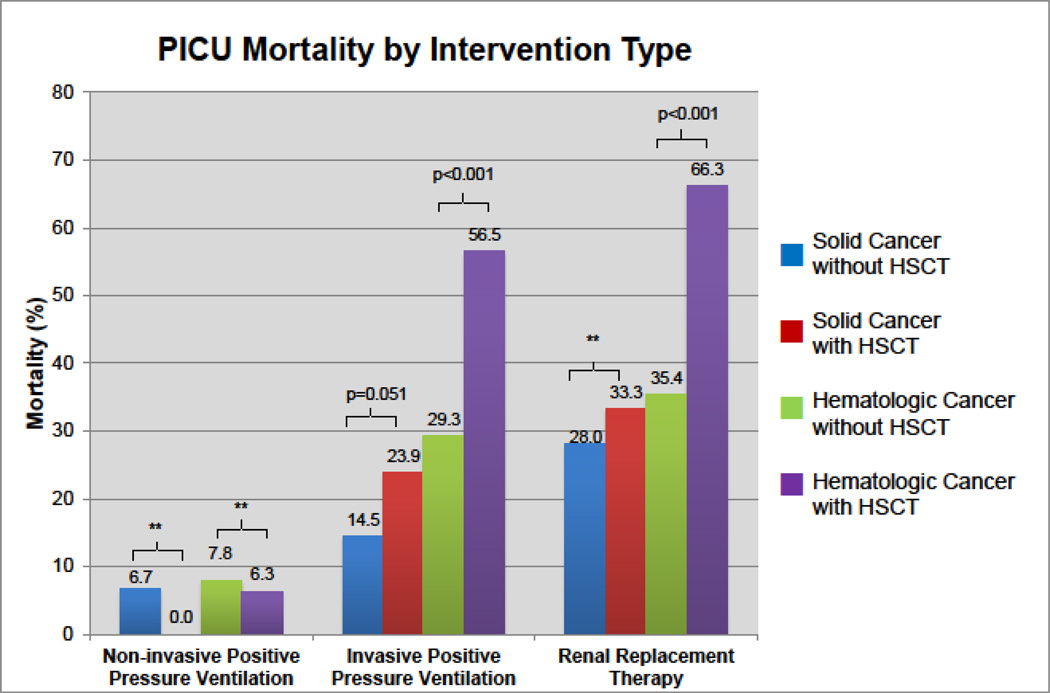
Results: After excluding scheduled perioperative admissions, cancer patients represented 4.2 % of all PICU admissions (10,365/246,346), had overall mortality of 6.8 % (708/10,365) vs. 2.4 % (5,485/230,548) in the general PICU population (RR = 2.9, 95 % CI 2.7-3.1, p < 0.001), and accounted for 11.4 % of all PICU deaths (708/6,215). Hematologic cancer patients had greater median PRISM3 score (8 vs 2, p < 0.001), rates of sepsis (27 vs 9 %, RR = 2.9, 95 % CI 2.6-3.1, p < 0.001), and mortality (9.6 vs 4.5 %, RR = 2.1, 95 % CI 1.8-2.5, p < 0.001) compared to solid cancer patients. Among hematologic cancer patients, stem cell transplantation, diagnosis of acute myeloid leukemia, PRISM3 score, and infection were all independently associated with PICU mortality.
Conclusions: Children with cancer account for 4.2 % of PICU admissions and 11.4 % of PICU deaths. Hematologic cancer patients have significantly higher admission illness severity, rates of infections, and PICU mortality than solid cancer patients. These data may be useful in risk stratification for closer monitoring and patient counseling.
Conflict of interest statement
Figures
Comment in
-
Optimism and no longer foolishness? Haematology/oncology and the PICU.Intensive Care Med. 2014 Oct;40(10):1589-91. doi: 10.1007/s00134-014-3478-2. Epub 2014 Sep 18. Intensive Care Med. 2014. PMID: 25231291 Free PMC article. No abstract available.
References
-
- National Cancer Institute. Surveillance, Epidemiology, and End Results (SEER) Program Research Data (1973–2011) DCCPS, Surveillance Research Program, Surveillance Systems Branch. 2014 doi: http://www.seer.cancer.gov.
-
- Dalton HJ, Slonim AD, Pollack MM. MultiCenter outcome of pediatric oncology patients requiring intensive care. Pediatr Hematol Oncol. 2003;20:643–649. - PubMed
-
- Rosenman MB, Vik T, Hui SL, Breitfeld PP. Hospital resource utilization in childhood cancer. J Pediatr Hematol Oncol. 2005;27:295–300. - PubMed
-
- Pollack MM, Patel KM, Ruttimann UE. PRISM III: an updated Pediatric Risk of Mortality score. Crit Care Med. 1996;24:743–752. - PubMed
-
- Tilford JM, Roberson PK, Lensing S, Fiser DH. Differences in pediatric ICU mortality risk over time. Crit Care Med. 1998;26:1737–1743. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
