

Fifteen-year survival outcomes following primary androgen-deprivation therapy for localized prostate cancer
- PMID: 25023796
- PMCID: PMC5499229
- DOI: 10.1001/jamainternmed.2014.3028
Fifteen-year survival outcomes following primary androgen-deprivation therapy for localized prostate cancer
Abstract
Importance: One in 6 American men will be diagnosed as having prostate cancer during their lifetime. Although there are no data to support the use of primary androgen-deprivation therapy (ADT) for early-stage prostate cancer, primary ADT has been widely used for localized prostate cancer, especially among older patients.
Objective: To determine the long-term survival impact of primary ADT in older men with localized (T1/T2) prostate cancer.
Design, setting, and participants: This was a population-based cohort study of 66,717 Medicare patients 66 years or older diagnosed from 1992 through 2009 who received no definitive local therapy within 180 days of prostate cancer diagnosis. The study was conducted in predefined US geographical areas covered by the Surveillance, Epidemiology, and End Results (SEER) Program. Instrumental variable analysis was used to assess the impact of primary ADT and control for potential biases associated with unmeasured confounding variables. The instrumental variable comprised combined health services areas with various usage rates of primary ADT. The analysis compared survival outcomes in the top tertile areas with those in the bottom tertile areas.
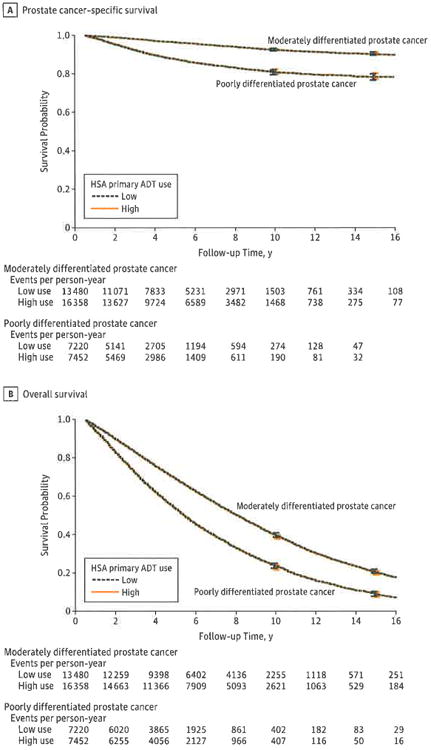
Main outcomes and measures: Prostate cancer-specific survival and overall survival.
Results: With a median follow-up of 110 months, primary ADT was not associated with improved 15-year overall or prostate cancer-specific survival following the diagnosis of localized prostate cancer. Among patients with moderately differentiated cancers, the 15-year overall survival was 20.0% in areas with high primary ADT use vs 20.8% in areas with low use (difference: 95% CI, -2.2% to 0.4%), and the 15-year prostate cancer survival was 90.6% in both high- and low-use areas (difference: 95% CI, -1.1% to 1.2%). Among patients with poorly differentiated cancers, the 15-year cancer-specific survival was 78.6% in high-use areas vs 78.5%, in low-use areas (difference: 95% CI, -1.8% to 2.4%), and the 15-year overall survival was 8.6% in high-use areas vs 9.2% in low-use areas (difference: 95% CI, -1.5% to 0.4%).
Conclusions and relevance: Primary ADT is not associated with improved long-term overall or disease-specific survival for men with localized prostate cancer. Primary ADT should be used only to palliate symptoms of disease or prevent imminent symptoms associated with disease progression.
Conflict of interest statement
Figures
Comment in
-
Measuring the effectiveness of androgen-deprivation therapy for prostate cancer in the medicare population: adequate data are neither the same as nor the enemy of perfect data.JAMA Intern Med. 2014 Sep;174(9):1468-9. doi: 10.1001/jamainternmed.2014.1107. JAMA Intern Med. 2014. PMID: 25023522 No abstract available.
-
Prostate cancer: Say no to ADT for localized disease.Nat Rev Urol. 2014 Sep;11(9):487. doi: 10.1038/nrurol.2014.187. Epub 2014 Jul 29. Nat Rev Urol. 2014. PMID: 25069734 No abstract available.
-
Prostate cancer: is androgen-deprivation therapy chosen wisely?Nat Rev Clin Oncol. 2014 Sep;11(9):501. doi: 10.1038/nrclinonc.2014.130. Epub 2014 Jul 29. Nat Rev Clin Oncol. 2014. PMID: 25073003 No abstract available.
References
-
- Cooperberg MR, Broering JM, Litwin MS, et al. CaPSURE Investigators. The contemporary management of prostate cancer in the United States: lessons from the cancer of the prostate strategic urologic research endeavor (CaPSURE), a national disease registry. J Urol. 2004;171(4):1393–1401. - PubMed
-
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. [Accessed January 30, 2013];Prostate Cancer. http://www.nccn.org/professionals/physician_gls/f_guidelines.asp#prostate.
-
- Shahinian VB, Kuo YF, Freeman JL, Orihuela E, Goodwin JS. Increasing use of gonadotropin-releasing hormone agonists for the treatment of localized prostate carcinoma. Cancer. 2005;103(8):1615–1624. - PubMed
-
- Studer UE, Collette L, Whelan P, et al. EORTC Genitourinary Group. Using PSA to guide timing of androgen deprivation in patients with TO-4 NO-2 MO prostate cancer not suitable for local curative treatment (EORTC 30891) Eur Urol. 2008;53(5):941–949. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
