

A prospective study of mediastinal gray-zone lymphoma
- PMID: 25024303
- PMCID: PMC4155269
- DOI: 10.1182/blood-2014-03-564906
A prospective study of mediastinal gray-zone lymphoma
Abstract
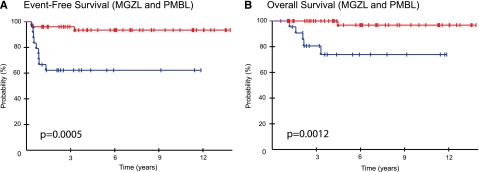
Mediastinal B-cell lymphomas present in the mediastinum and are most frequent in young patients. Nodular sclerosis Hodgkin lymphoma (NSHL) and primary mediastinal B-cell lymphoma (PMBL) are the common types, whereas mediastinal gray-zone lymphoma (MGZL) is extremely rare and has pathological features intermediate between NSHL and PMBL. The indeterminate pathobiology of MGZL has led to uncertainty regarding therapeutic strategy, and its clinical characteristics and treatment have not been characterized. We conducted a prospective study of infusional dose-adjusted etoposide, doxorubicin, and cyclophosphamide with vincristine, prednisone, and rituximab (DA-EPOCH-R) and filgrastim in untreated MGZL. We analyzed biomarkers of outcome and compared their clinical and biological characteristics to PMBL. Twenty-four MGZL patients had a median age of 33 years (range, 14 to 59 years), and 46% had mediastinal masses ≥10 cm. At 59 months median follow-up, the event-free survival and overall survival were 62% and 74%, respectively. The serum absolute lymphocyte count, the presence of tumor-infiltrating dendritic cells, CD15 expression on the malignant cells, and tumor morphology were biomarkers of outcome in MGZL. Compared with PMBL, MGZL patients were more likely to be male, express CD15, have lower expression of CD20, and have a worse outcome. DA-EPOCH-R alone is effective in MGZL. The trial was registered at ClinicalTrials.gov (NCT00001337).
Figures


References
-
- Savage KJ, Monti S, Kutok JL, et al. The molecular signature of mediastinal large B-cell lymphoma differs from that of other diffuse large B-cell lymphomas and shares features with classical Hodgkin lymphoma. Blood. 2003;102(12):3871–3879. - PubMed
-
- Swerdlow S, Harris NL, Campo E, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed. Lyon: International Agency for Research on Cancer; 2008.
-
- Traverse-Glehen A, Pittaluga S, Gaulard P, et al. Mediastinal gray zone lymphoma: the missing link between classic Hodgkin’s lymphoma and mediastinal large B-cell lymphoma. Am J Surg Pathol. 2005;29(11):1411–1421. - PubMed
-
- Quintanilla-Martinez L, de Jong D, de Mascarel A, et al. Gray zones around diffuse large B cell lymphoma. Conclusions based on the workshop of the XIV meeting of the European Association for Hematopathology and the Society of Hematopathology in Bordeaux, France. J Hematop. 2009;2(4):211–236. - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
