

Quality of vitamin K antagonist control and outcomes in atrial fibrillation patients: a meta-analysis and meta-regression
- PMID: 25024644
- PMCID: PMC4094926
- DOI: 10.1186/1477-9560-12-14
Quality of vitamin K antagonist control and outcomes in atrial fibrillation patients: a meta-analysis and meta-regression
Abstract
Background: Atrial fibrillation (AF) patients frequently require anticoagulation with vitamin K antagonists (VKAs) to prevent thromboembolic events, but their use increases the risk of hemorrhage. We evaluated time spent in therapeutic range (TTR), proportion of international normalized ratio (INR) measurements in range (PINRR), adverse events in relation to INR, and predictors of INR control in AF patients using VKAs.
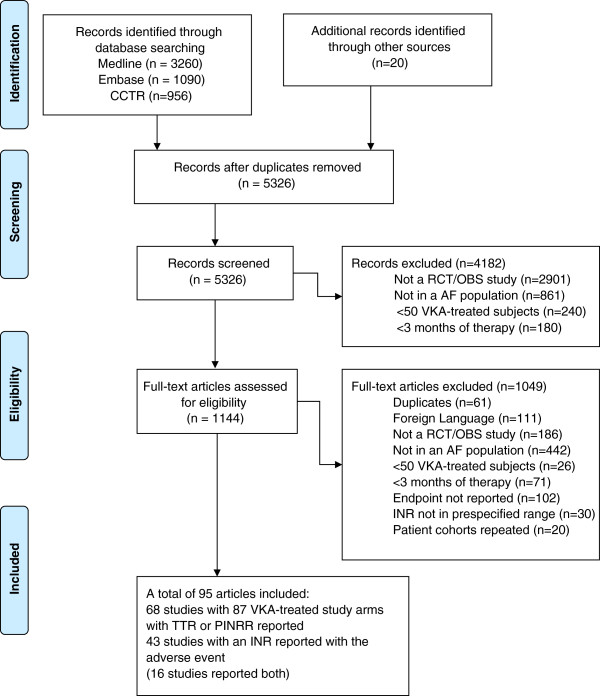
Methods: We searched MEDLINE, CENTRAL and EMBASE (1990-June 2013) for studies of AF patients receiving adjusted-dose VKAs that reported INR control measures (TTR and PINRR) and/or reported an INR measurement coinciding with thromboembolic or hemorrhagic events. Random-effects meta-analyses and meta-regression were performed.
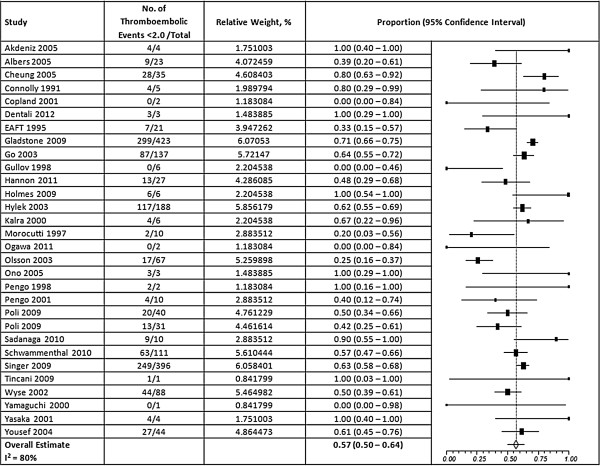
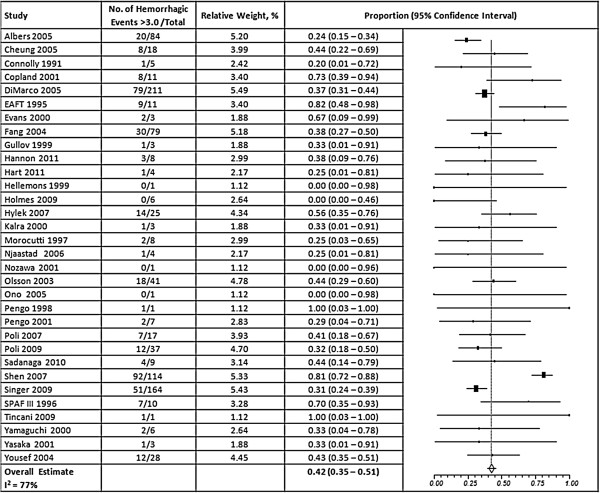
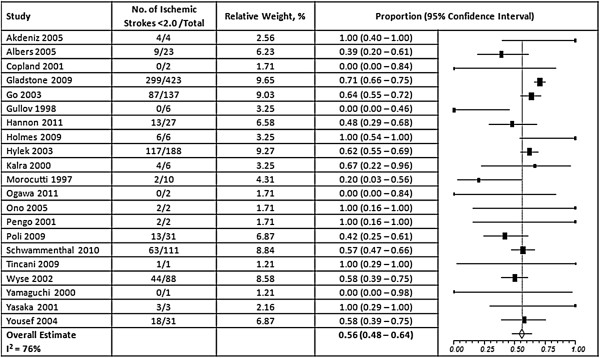
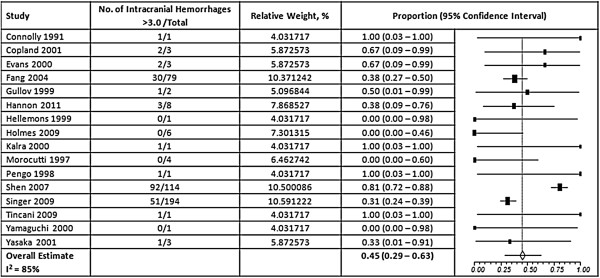
Results: Ninety-five articles were included. Sixty-eight VKA-treated study groups reported measures of INR control, while 43 studies reported an INR around the time of the adverse event. Patients spent 61% (95% CI, 59-62%), 25% (95% CI, 23-27%) and 14% (95% CI, 13-15%) of their time within, below or above the therapeutic range. PINRR assessments were within, below, and above range 56% (95% CI, 53-59%), 26% (95% CI, 23-29%) and 13% (95% CI, 11-17%) of the time. Patients receiving VKA management in the community spent less TTR than those managed by anticoagulation clinics or in randomized trials. Patients newly receiving VKAs spent less TTR than those with prior VKA use. Patients in Europe/United Kingdom spent more TTR than patients in North America. Fifty-seven percent (95% CI, 50-64%) of thromboembolic events and 42% (95% CI, 35 - 51%) of hemorrhagic events occurred at an INR <2.0 and >3.0, respectively; while 56% (95% CI, 48-64%) of ischemic strokes and 45% of intracranial hemorrhages (95% CI, 29-63%) occurred at INRs <2.0 and >3.0, respectively.
Conclusions: Patients on VKAs for AF frequently have INRs outside the therapeutic range. While, thromboembolic and hemorrhagic events do occur patients with a therapeutic INR; patients with an INR <2.0 make up many of the cases of thromboembolism, while those >3.0 make up many of the cases of hemorrhage. Managing anticoagulation outside of a clinical trial or anticoagulation clinic is associated with poorer INR control, as is, the initiation of therapy in the VKA-naïve. Patients in Europe/UK have better INR control than those in North America.
Keywords: Anticoagulation; Atrial fibrillation; International normalized ratio; Vitamin K antagonists.
Figures
References
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation: a major contributor to stroke in the elderly: the Framingham Heart Study. Arch Intern Med. 1987;147(9):1561–1564. - PubMed
-
- Atrial Fibrillation Investigators. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Analysis of pooled data from five randomized controlled trials. Arch Intern Med. 1994;154(13):1449–1457. - PubMed
-
- Fuster V, Rydén LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, Halperin JL, Le Heuzey JY, Kay GN, Lowe JE, Olsson SB, Prystowsky EN, Tamargo JL, Wann S, Smith SC Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Halperin JL, Hunt SA, Nishimura R, Ornato JP, Page RL, Riegel B, Priori SG, Blanc JJ, Budaj A, Camm AJ, Dean V, Deckers JW, Despres C, Dickstein K, Lekakis J, McGregor K, Metra M, Morais J, Osterspey A, Tamargo JL, Zamorano JL. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation. Circulation. 2006;114(7):e257–e354. - PubMed
-
- Singer DE, Albers GW, Dalen JE, Fang MC, Go AS, Halperin JL, Lip GY, Manning WJ. American College of Chest Physicians. Antithrombotic therapy in atrial fibrillation: American college of chest physicians evidence-based clinical practice guidelines (8th Edition) Chest. 2008;133(6 Suppl):546S–592S. - PubMed
-
- Ansell J, Hirsh J, Hylek E, Jacobson A, Crowther M, Palareti G. American College of Chest Physicians. Pharmacology and management of the vitamin K antagonists: American college of chest physicians evidence-based clinical practice guidelines (8th Edition) Chest. 2008;133(6 Suppl):160S–198S. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
