

Rising rates of carbapenem-resistant enterobacteriaceae in community hospitals: a mixed-methods review of epidemiology and microbiology practices in a network of community hospitals in the southeastern United States
- PMID: 25026612
- PMCID: PMC4217156
- DOI: 10.1086/677157
Rising rates of carbapenem-resistant enterobacteriaceae in community hospitals: a mixed-methods review of epidemiology and microbiology practices in a network of community hospitals in the southeastern United States
Abstract
Objective: Describe the epidemiology of carbapenem-resistant Enterobacteriaceae (CRE) and examine the effect of lower carbapenem breakpoints on CRE detection.
Design: Retrospective cohort.
Setting: Inpatient care at community hospitals.
Patients: All patients with CRE-positive cultures were included.
Methods: CRE isolated from 25 community hospitals were prospectively entered into a centralized database from January 2008 through December 2012. Microbiology laboratory practices were assessed using questionnaires.
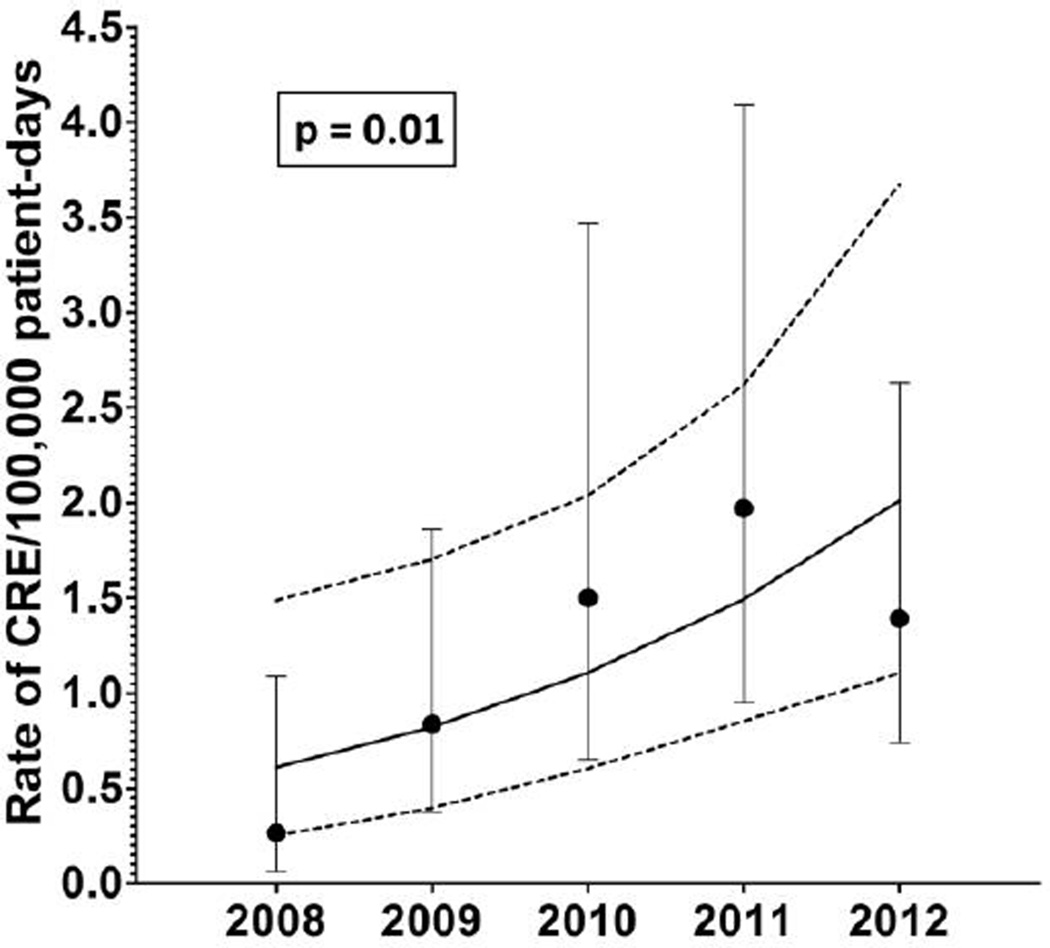
Results: A total of 305 CRE isolates were detected at 16 hospitals (64%). Patients with CRE had symptomatic infection in 180 cases (59%) and asymptomatic colonization in the remainder (125 cases; 41%). Klebsiella pneumoniae (277 isolates; 91%) was the most prevalent species. The majority of cases were healthcare associated (288 cases; 94%). The rate of CRE detection increased more than fivefold from 2008 (0.26 cases per 100,000 patient-days) to 2012 (1.4 cases per 100,000 patient-days; incidence rate ratio (IRR), 5.3 [95% confidence interval (CI), 1.22-22.7]; P = .01). Only 5 hospitals (20%) had adopted the 2010 Clinical and Laboratory Standards Institute (CLSI) carbapenem breakpoints. The 5 hospitals that adopted the lower carbapenem breakpoints were more likely to detect CRE after implementation of breakpoints than before (4.1 vs 0.5 cases per 100,000 patient-days; P < .001; IRR, 8.1 [95% CI, 2.7-24.6]). Hospitals that implemented the lower carbapenem breakpoints were more likely to detect CRE than were hospitals that did not (3.3 vs 1.1 cases per 100,000 patient-days; P = .01).
Conclusions: The rate of CRE detection increased fivefold in community hospitals in the southeastern United States from 2008 to 2012. Despite this, our estimates are likely underestimates of the true rate of CRE detection, given the low adoption of the carbapenem breakpoints recommended in the 2010 CLSI guidelines.
Conflict of interest statement
Figures
Comment in
-
Much to do about carbapenem-resistant Enterobacteriaceae: why supplementing surveillance may be the key to stopping spread.Infect Control Hosp Epidemiol. 2014 Aug;35(8):984-5. doi: 10.1086/677158. Epub 2014 Jun 20. Infect Control Hosp Epidemiol. 2014. PMID: 25026613 No abstract available.
References
-
- Ben-David D, Kordevani R, Keller N, et al. Outcome of carbapenem resistant Klebsiella pneumoniae bloodstream infections. Clin Microbiol Infect. 2012;18(1):54–60. - PubMed
-
- Borer A, Saidel-Odes L, Riesenberg K, et al. Attributable mortality rate for carbapenem-resistant Klebsiella pneumoniae bacteremia. Infect Control Hosp Epidemiol. 2009;30(10):972–976. - PubMed
-
- Patel G, Huprikar S, Factor SH, Jenkins SG, Calfee DP. Outcomes of carbapenem-resistant Klebsiella pneumoniae infection and the impact of antimicrobial and adjunctive therapies. Infect Control Hosp Epidemiol. 2008;29(12):1099–1106. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources