

Pharmacometabolomics reveals that serotonin is implicated in aspirin response variability
- PMID: 25029353
- PMCID: PMC4120016
- DOI: 10.1038/psp.2014.22
Pharmacometabolomics reveals that serotonin is implicated in aspirin response variability
Abstract
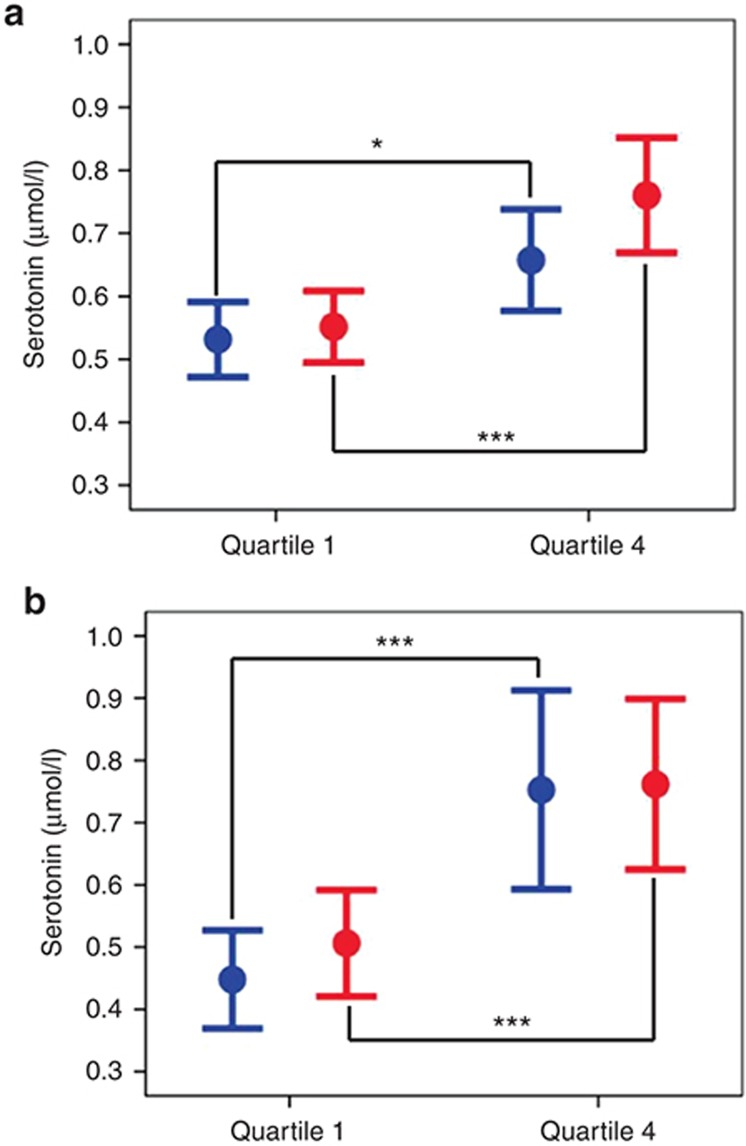
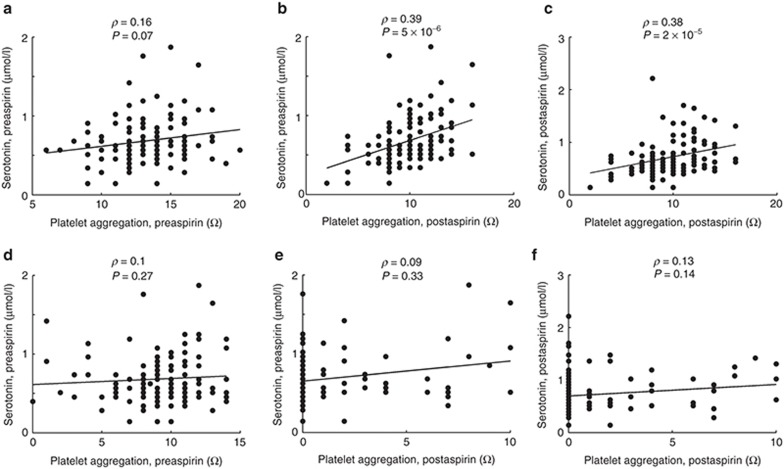
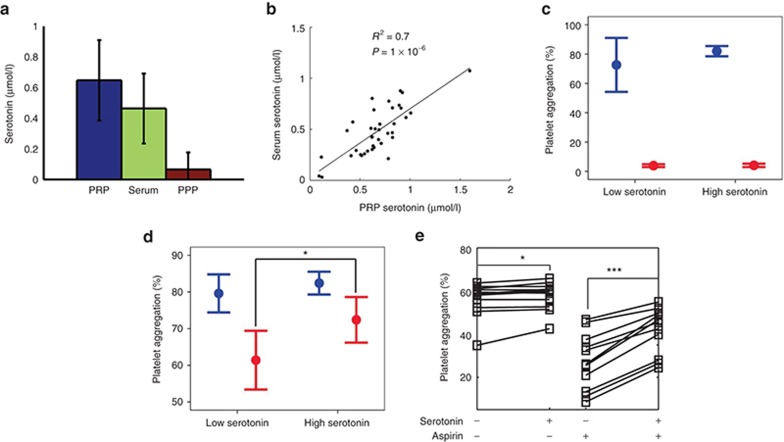
While aspirin is generally effective for prevention of cardiovascular disease, considerable variation in drug response exists, resulting in some individuals displaying high on-treatment platelet reactivity. We used pharmacometabolomics to define pathways implicated in variation of response to treatment. We profiled serum samples from healthy subjects pre- and postaspirin (14 days, 81 mg/day) using mass spectrometry. We established a strong signature of aspirin exposure independent of response (15/34 metabolites changed). In our discovery (N = 80) and replication (N = 125) cohorts, higher serotonin levels pre- and postaspirin correlated with high, postaspirin, collagen-induced platelet aggregation. In a third cohort, platelets from subjects with the highest levels of serotonin preaspirin retained higher reactivity after incubation with aspirin than platelets from subjects with the lowest serotonin levels preaspirin (72 ± 8 vs. 61 ± 11%, P = 0.02, N = 20). Finally, ex vivo, serotonin strongly increased platelet reactivity after platelet incubation with aspirin (+20%, P = 4.9 × 10(-4), N = 12). These results suggest that serotonin is implicated in aspirin response variability.
Figures
References
-
- Hovens M.M., Snoep J.D., Eikenboom J.C., van der Bom J.G., Mertens B.J., Huisman M.V. Prevalence of persistent platelet reactivity despite use of aspirin: a systematic review. Am. Heart J. 2007;153:175–181. - PubMed
-
- Gum P.A., Kottke-Marchant K., Welsh P.A., White J., Topol E.J. A prospective, blinded determination of the natural history of aspirin resistance among stable patients with cardiovascular disease. J. Am. Coll. Cardiol. 2003;41:961–965. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
