

Benefit of cup medialization in total hip arthroplasty is associated with femoral anatomy
- PMID: 25030101
- PMCID: PMC4160515
- DOI: 10.1007/s11999-014-3787-3
Benefit of cup medialization in total hip arthroplasty is associated with femoral anatomy
Abstract
Background: Medialization of the cup with a respective increase in femoral offset has been proposed in THA to increase abductor moment arms. Insofar as there are potential disadvantages to cup medialization, it is important to ascertain whether the purported biomechanical benefits of cup medialization are large enough to warrant the downsides; to date, studies regarding this question have disagreed.
Questions/purposes: The purpose of this study was to quantify the effect of cup medialization with a compensatory increase in femoral offset compared with anatomic reconstruction for patients undergoing THA. We tested the hypothesis that there is a (linear) correlation between preoperative anatomic parameters and muscle moment arm increase caused by cup medialization.
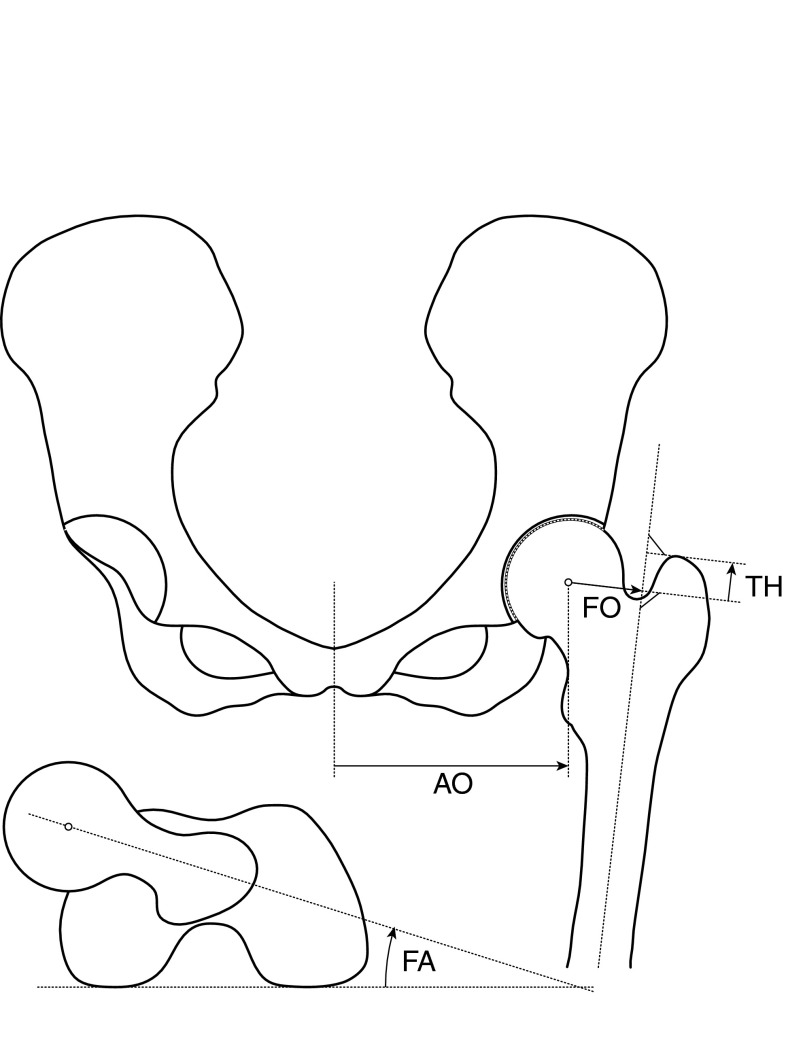
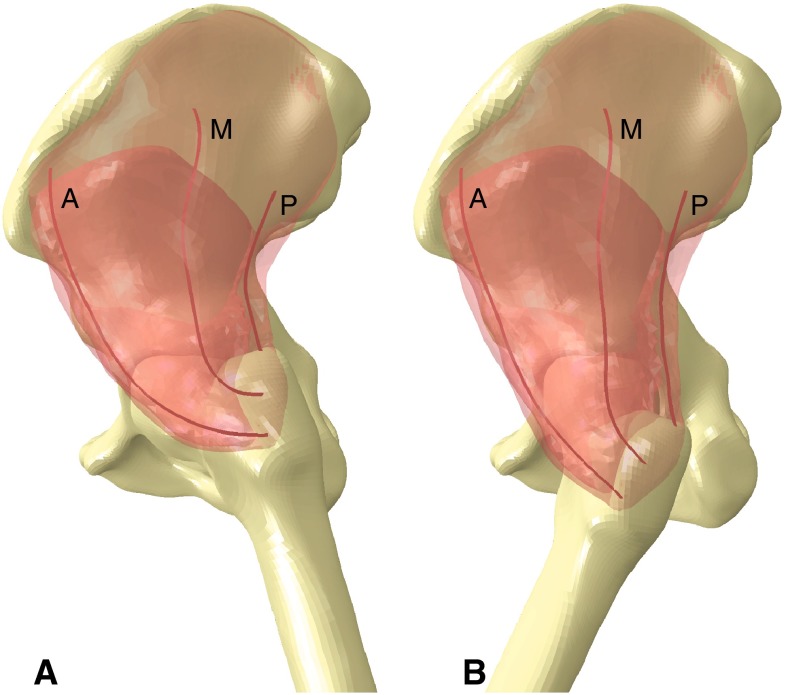
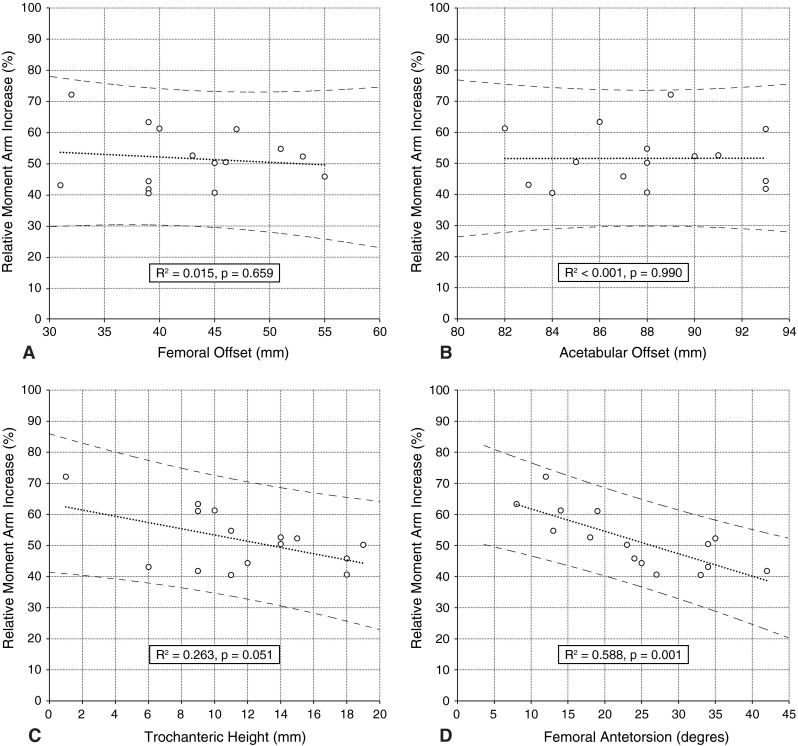
Methods: Fifteen patients undergoing THA were selected, covering a typical range of preoperative femoral offsets. For each patient, a finite element model was built based on a preoperative CT scan. The model included the pelvis, femur, gluteus minimus, medius, and maximus. Two reconstructions were compared: (1) anatomic position of the acetabular center of rotation, and (2) cup medialization compensated by an increase in the femoral offset. Passive abduction-adduction and flexion-extension were simulated in the range of normal gait. Muscle moment arms were evaluated and correlated to preoperative femoral offset, acetabular offset, height of the greater trochanter (relative to femoral center of rotation), and femoral antetorsion angle.
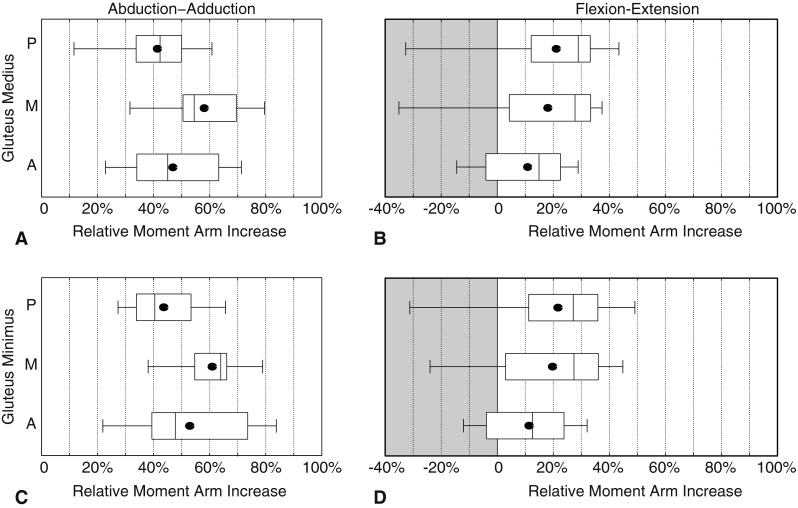
Results: The increase of muscle moment arms caused by cup medialization varied among patients. Muscle moment arms increase by 10% to 85% of the amount of cup medialization for abduction-adduction and from -35% (decrease) to 50% for flexion-extension. The change in moment arm was inversely correlated (R(2) = 0.588, p = 0.001) to femoral antetorsion (anteversion), such that patients with less femoral antetorsion gained more in terms of hip muscle moments. No linear correlation was observed between changes in moment arm and other preoperative parameters in this series.
Conclusions: The benefit of cup medialization is variable and depends on the individual anatomy.
Clinical relevance: Cup medialization with compensatory increase of the femoral offset may be particularly effective in patients with less femoral antetorsion. However, cup medialization must be balanced against its tradeoffs, including the additional loss of medial acetabular bone stock, and eventual proprioceptive implications of the nonanatomic center of rotation and perhaps joint reaction forces. Clinical studies should better determine the relevance of small changes of moment arms on function and joint reaction forces.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
