

Development of antibiotic treatment algorithms based on local ecology and respiratory surveillance cultures to restrict the use of broad-spectrum antimicrobial drugs in the treatment of hospital-acquired pneumonia in the intensive care unit: a retrospective analysis
- PMID: 25030270
- PMCID: PMC4223549
- DOI: 10.1186/cc13990
Development of antibiotic treatment algorithms based on local ecology and respiratory surveillance cultures to restrict the use of broad-spectrum antimicrobial drugs in the treatment of hospital-acquired pneumonia in the intensive care unit: a retrospective analysis
Abstract
Introduction: Timely administration of appropriate antibiotic therapy has been shown to improve outcome in hospital-acquired pneumonia (HAP). Empirical treatment guidelines tailored to local ecology have been advocated in antibiotic stewardship programs. We compared a local ecology based algorithm (LEBA) to a surveillance culture based algorithm (SCBA) in terms of appropriate coverage and spectrum of antimicrobial activity.
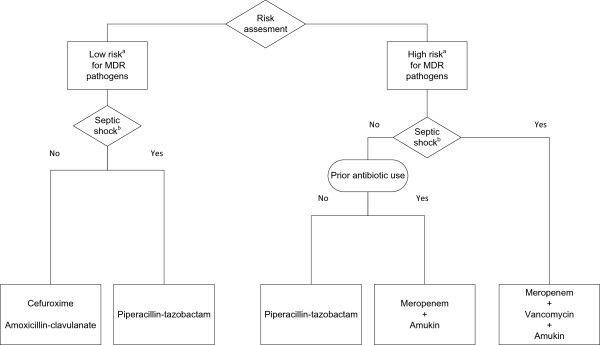
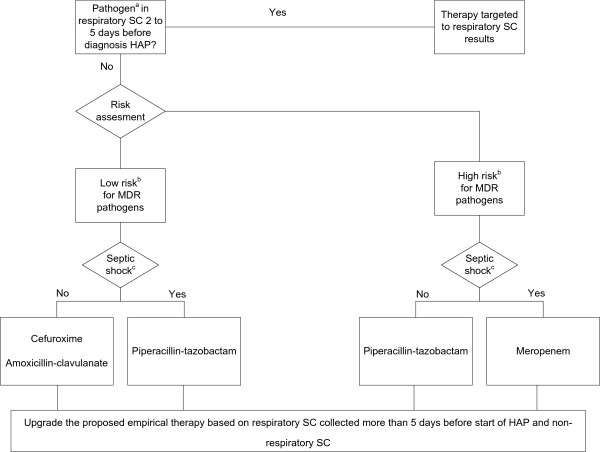
Methods: We retrospectively assessed 2 hypothetical empirical antibiotic treatment algorithms for HAP on an existing high-quality prospectively collected database in a mixed 36-bed tertiary intensive care unit (ICU). Data on consecutive episodes of microbiologically confirmed HAP were collected over a period of 40 months and divided in a derivation (1 July 2009 to 31 October 2010) and validation (1 November 2010 until 31 October 2012) cohort. On the derivation cohort we constructed a LEBA, based on overall observed bacterial resistance patterns, and a SCBA, which targeted therapy to surveillance culture (SC) in the individual patient. Therapy was directed against pathogens found in respiratory SC collected two to five days before HAP, and in the absence of these, presence or absence of multi-drug resistant (MDR) pathogens in other SC dictated broad-spectrum, respectively narrow spectrum antibiotic therapy. Subsequently, LEBA and SCBA were retrospectively reviewed and compared with actually prescribed antibiotics in the validation cohort.
Results: The first 100 HAP episodes made up the derivation cohort and the subsequent 113 HAP episodes the validation cohort. Appropriate antibiotic coverage rates by applying LEBA and SCBA were 88.5% and 87.6%, respectively, and did not differ significantly with respect to appropriateness of the actually prescribed initial therapy (84.1%). SCBA proposed more narrow spectrum therapy as compared to LEBA and the actually prescribed antimicrobials (P <0.001). SCBA recommended significantly less combination therapy and carbapenems compared to LEBA (P <0.001). SCBA targeted antibiotics to recent respiratory SC in 38.1% (43 out of 113 episodes) of HAP; in these cases adequacy was 93% (40 out of 43).
Conclusion: Rates of appropriate antimicrobial coverage were identical in LEBA and SCBA. However, in this setting of moderate MDR prevalence, the use of SCBA would result in a significant reduction of the use of broad-spectrum drugs and may be a preferential strategy when implementing antibiotic stewardship programs.
Figures

Comment in
-
Minimizing antibiotic exposure in the ICU: in search of the optimal strategy.Crit Care. 2014 Oct 31;18(5):613. doi: 10.1186/s13054-014-0613-y. Crit Care. 2014. PMID: 25672663 Free PMC article.
References
-
- Policy statement on antimicrobial stewardship by the Society for Healthcare Epidemiology of America (SHEA), the Infectious Diseases Society of America (IDSA), and the Pediatric Infectious Diseases Society (PIDS) Infect Control Hosp Epidemiol. 2012;33:322–327. - PubMed
-
- ᅟ. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171:388–416. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
