

Risk factors for serrated polyps of the colorectum
- PMID: 25030942
- PMCID: PMC4881384
- DOI: 10.1007/s10620-014-3277-1
Risk factors for serrated polyps of the colorectum
Abstract
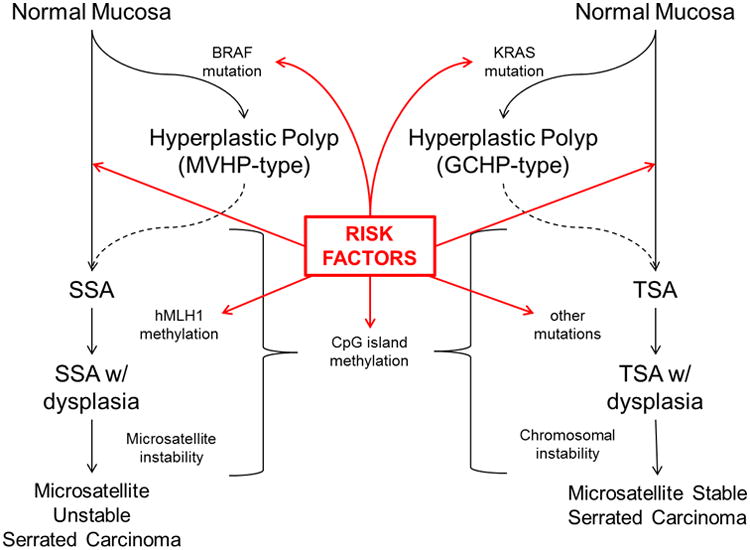
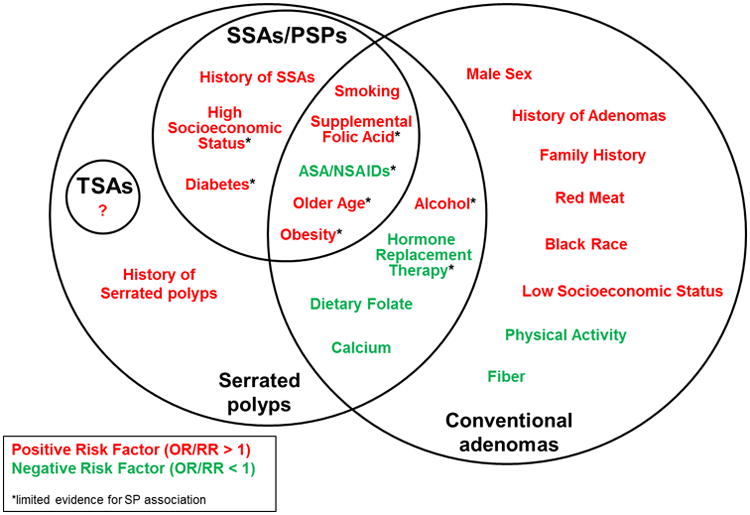
Serrated pathway polyps are a relatively new area of interest in the field of colorectal cancer screening and prevention. Akin to conventional adenomas, some serrated polyps (SPs) have the potential to develop into malignant serrated neoplasms, yet little is known regarding risk factors for these lesions. Early epidemiological studies of hyperplastic polyps were performed without knowledge of the serrated pathway and likely included a mixture of SPs. More recently, studies have specifically evaluated premalignant SPs, such as the sessile serrated adenoma (SSA) or surrogates for these polyps such as large or proximally located SPs. SPs share some risk factors with conventional adenomas and have been associated with tobacco use, obesity, and age. Nonsteroidal anti-inflammatory drug (NSAID) use, fiber, folic acid, and calcium have been associated with reduced risk of SPs. Studies focused on SSAs specifically have reported associations with age, female sex, smoking, obesity, diabetes, and possibly diets high in fat, carbohydrates, and calories. Higher education has also been associated with risk of SSAs, while an inverse association between NSAID use and SSAs has been reported. Risk factors for traditional serrated adenomas are largely unknown. Studies are largely limited by varying inclusion criteria, as well as differences in pathological classification schemes. Further epidemiological studies of SPs are needed to aid in risk stratification and screening, and etiological research.
Figures
References
-
- Morson B. Some peculiarities in the histology of intestinal polyps. Dis Colon Rectum. 1962;5:337–44.
-
- Oka S, Tanaka S, Hiyama T, et al. Clinicopathologic and endoscopic features of colorectal serrated adenoma: differences between polypoid and superficial types. Gastrointest Endosc. 2004;59(2):213–9. - PubMed
-
- Huang CS, Farraye FA, Yang S, et al. The clinical significance of serrated polyps. Am J Gastroenterol. 2011;106(2):229–40. quiz 241. - PubMed
-
- Pohl H, Srivastava A, Bensen SP, et al. Incomplete polyp resection during colonoscopy-results of the complete adenoma resection (CARE) study. Gastroenterology. 2013;144(1):74–80 e1. - PubMed
-
- Hetzel JT, Huang CS, Coukos JA, et al. Variation in the detection of serrated polyps in an average risk colorectal cancer screening cohort. Am J Gastroenterol. 2010;105(12):2656–64. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
