

Neurocognitive outcome of children exposed to perinatal mother-to-child Chikungunya virus infection: the CHIMERE cohort study on Reunion Island
- PMID: 25033077
- PMCID: PMC4102444
- DOI: 10.1371/journal.pntd.0002996
Neurocognitive outcome of children exposed to perinatal mother-to-child Chikungunya virus infection: the CHIMERE cohort study on Reunion Island
Abstract
Background: Little is known about the neurocognitive outcome in children exposed to perinatal mother-to-child Chikungunya virus (p-CHIKV) infection.
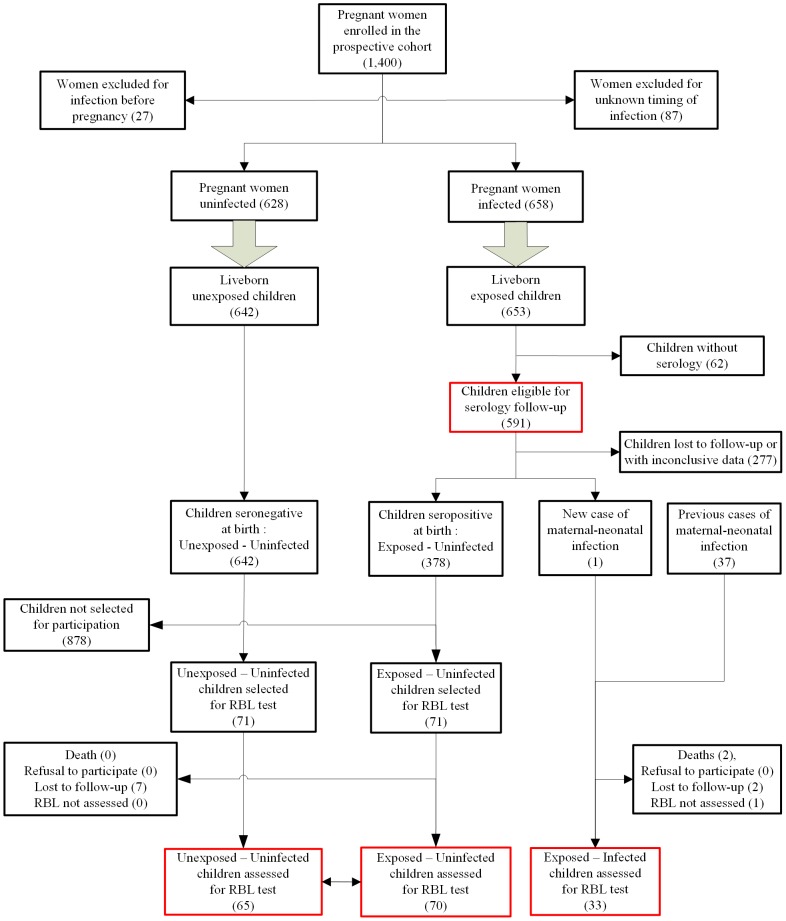
Methods: The CHIMERE ambispective cohort study compared the neurocognitive function of 33 p-CHIKV-infected children (all but one enrolled retrospectively) at around two years of age with 135 uninfected peers (all enrolled prospectively). Psychomotor development was assessed using the revised Brunet-Lezine scale, examiners blinded to infectious status. Development quotients (DQ) with subscores covering movement/posture, coordination, language, sociability skills were calculated. Predictors of global neurodevelopmental delay (GND, DQ ≤ 85), were investigated using multivariate Poisson regression modeling. Neuroradiologic follow-up using magnetic resonance imaging (MRI) scans was proposed for most of the children with severe forms.
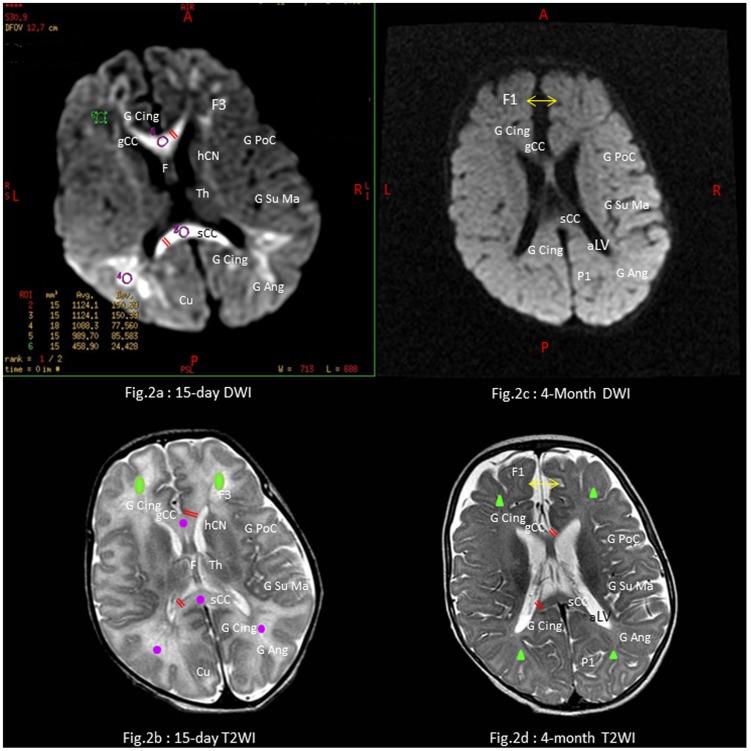
Results: The mean DQ score was 86.3 (95%CI: 81.0-91.5) in infected children compared to 100.2 (95%CI: 98.0-102.5) in uninfected peers (P<0.001). Fifty-one percent (n = 17) of infected children had a GND compared to 15% (n = 21) of uninfected children (P<0.001). Specific neurocognitive delays in p-CHIKV-infected children were as follows: coordination and language (57%), sociability (36%), movement/posture (27%). After adjustment for maternal social situation, small for gestational age, and head circumference, p-CHIKV infection was found associated with GND (incidence rate ratio: 2.79, 95%CI: 1.45-5.34). Further adjustments on gestational age or breastfeeding did not change the independent effect of CHIKV infection on neurocognitive outcome. The mean DQ of p-CHIKV-infected children was lower in severe encephalopathic children than in non-severe children (77.6 versus 91.2, P<0.001). Of the 12 cases of CHIKV neonatal encephalopathy, five developed a microcephaly (head circumference <-2 standard deviations) and four matched the definition of cerebral palsy. MRI scans showed severe restrictions of white matter areas, predominant in the frontal lobes in these children.
Conclusions: The neurocognitive outcome of children exposed to perinatal mother-to-child CHIKV infection is poor. Severe CHIKV neonatal encephalopathy is associated with an even poorer outcome.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Staples JE, Breiman RF, Powers AM (2009) Chikungunya fever: an epidemiological review of a reemerging infectious disease. Clin Infect Dis 49: 942–948. - PubMed
-
- Rezza G, Nicoletti L, Angelini R, Romi R, Finarelli AC, et al. (2007) Infection with Chikungunya virus in Italy: an outbreak in a temperate region. Lancet 370: 1840–1846. - PubMed
-
- Lemant J, Boisson V, Winer A, Thibault L, André H, et al. (2008) Serious acute chikungunya virus infection requiring intensive care during the Reunion Island outbreak in 2005–2006. Crit Care Med 36: 2536–2541. - PubMed
-
- Economopoulou A, Dominguez M, Helynck B, Sissoko D, Wichmann O, et al. (2009) Atypical Chikungunya virus infections: clinical manifestations, mortality and risk factors for severe disease during the 2005–2006 outbreak on Reunion. Epidemiol Infect 137: 534–541. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
