

Extracorporeal carbon dioxide removal for patients with acute respiratory failure secondary to the acute respiratory distress syndrome: a systematic review
- PMID: 25033302
- PMCID: PMC4056779
- DOI: 10.1186/cc13875
Extracorporeal carbon dioxide removal for patients with acute respiratory failure secondary to the acute respiratory distress syndrome: a systematic review
Abstract
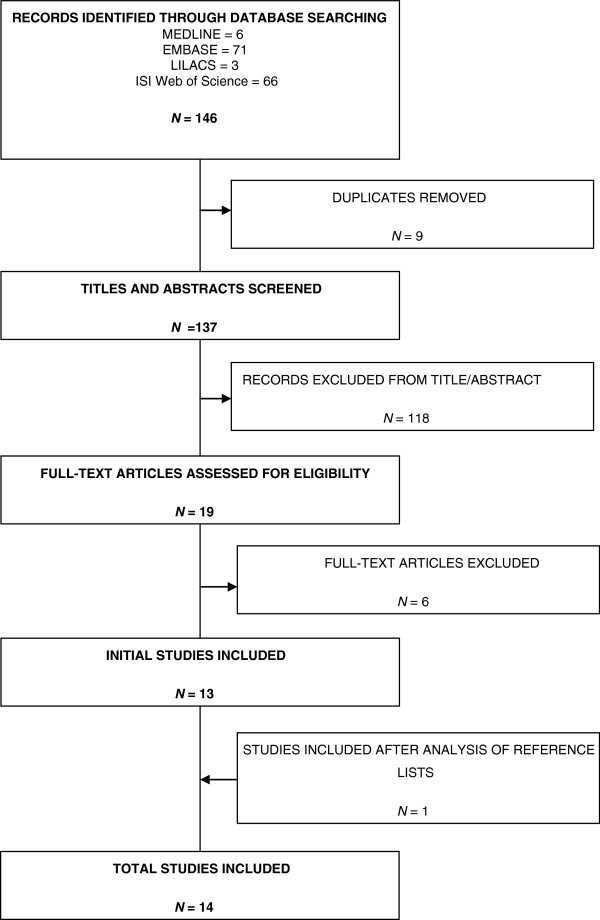
Acute respiratory distress syndrome (ARDS) continues to have significant mortality and morbidity. The only intervention proven to reduce mortality is the use of lung-protective mechanical ventilation strategies, although such a strategy may lead to problematic hypercapnia. Extracorporeal carbon dioxide removal (ECCO₂R) devices allow uncoupling of ventilation from oxygenation, thereby removing carbon dioxide and facilitating lower tidal volume ventilation. We performed a systematic review to assess efficacy, complication rates, and utility of ECCO₂R devices. We included randomised controlled trials (RCTs), case-control studies and case series with 10 or more patients. We searched MEDLINE, Embase, LILACS (Literatura Latino Americana em Ciências da Saúde), and ISI Web of Science, in addition to grey literature and clinical trials registries. Data were independently extracted by two reviewers against predefined criteria and agreement was reached by consensus. Outcomes of interest included mortality, intensive care and hospital lengths of stay, respiratory parameters and complications. The review included 14 studies with 495 patients (two RCTs and 12 observational studies). Arteriovenous ECCO₂R was used in seven studies, and venovenous ECCO₂R in seven studies. Available evidence suggests no mortality benefit to ECCO₂R, although post hoc analysis of data from the most recent RCT showed an improvement in ventilator-free days in more severe ARDS. Organ failure-free days or ICU stay have not been shown to decrease with ECCOvR. Carbon dioxide removal was widely demonstrated as feasible, facilitating the use of lower tidal volume ventilation. Complication rates varied greatly across the included studies, representing technological advances. There was a general paucity of high-quality data and significant variation in both practice and technology used among studies, which confounded analysis. ECCO₂R is a rapidly evolving technology and is an efficacious treatment to enable protective lung ventilation. Evidence for a positive effect on mortality and other important clinical outcomes is lacking. Rapid technological advances have led to major changes in these devices and together with variation in study design have limited applicability of analysis. Further well-designed adequately powered RCTs are needed.
Figures
References
-
- Villar J, Blanco J, Anon JM, Santos-Bouza A, Blanch L, Ambros A, Gandia F, Carriedo D, Mosteiro F, Basaldua S, Fernandez RL, Kacmarek RM. ALIEN Network. The ALIEN study: incidence and outcome of acute respiratory distress syndrome in the era of lung protective ventilation. Intensive Care Med. 2011;37:1932–1941. doi: 10.1007/s00134-011-2380-4. - DOI - PubMed
-
- ARDS Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–1308. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
