

Central venous pressure after coronary artery bypass surgery: does it predict postoperative mortality or renal failure?
- PMID: 25035048
- PMCID: PMC4315310
- DOI: 10.1016/j.jcrc.2014.05.027
Central venous pressure after coronary artery bypass surgery: does it predict postoperative mortality or renal failure?
Abstract
Objective: Although hemodynamic monitoring is often performed after coronary artery bypass grafting (CABG), the role of monitoring postoperative central venous pressure (CVP) measurement as a predictor of clinical outcomes is unknown. As such, this study tests the hypothesis that postoperative CVP is predictive of operative mortality or renal failure.
Methods: This is an observational cohort study of detailed clinical data from 2390 randomly selected patients undergoing high-risk CABG or CABG/valve at 55 hospitals participating in the Society of Thoracic Surgeons' National Cardiac Surgery Database 2004-2005. Eligible patients underwent elective/urgent CABG with an ejection fraction less than 40% or elective/urgent CABG at 65 years or older with diabetes or a glomerular filtration rate less than 60 mL/min per 1.73 m2. The exposure of interest is CVP monitoring in the intensive care unit after adult cardiac surgery. The primary outcome measure was correlation between postoperative CVP and inhospital/30-day mortality and renal failure, assessed as a continuous variable, both unadjusted and after adjusting for important clinical factors using logistic regression modeling.
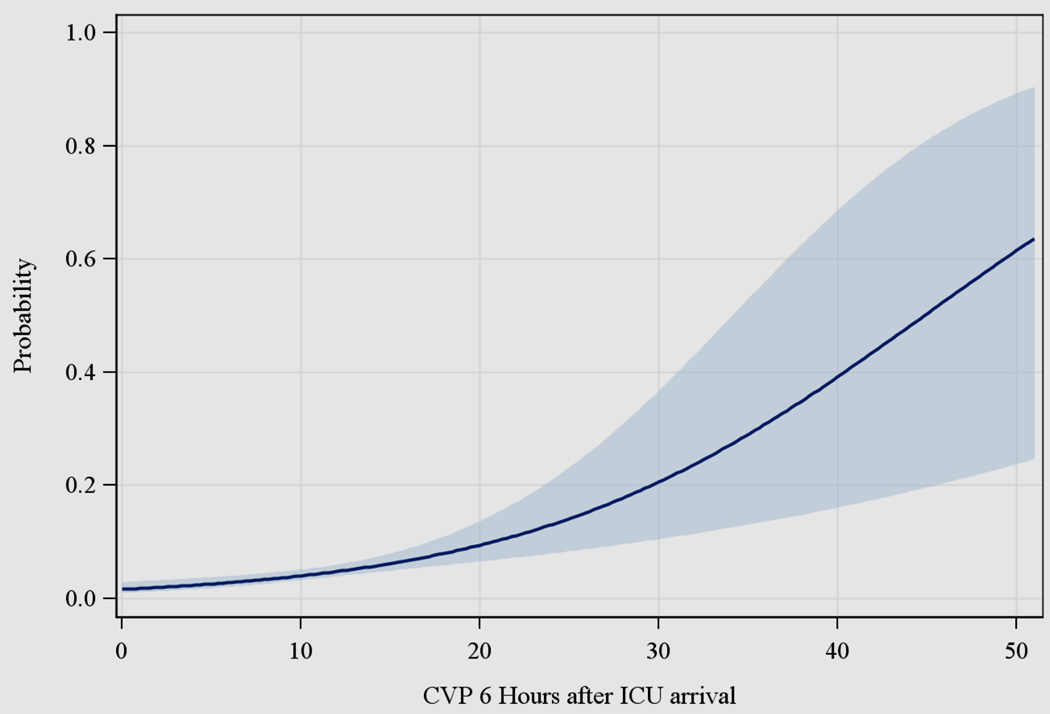
Results: Mean age was 72 years, 54% of patients had diabetes mellitus, 49% were urgent procedures, and mean cardiopulmonary bypass time was 105 minutes. Patients' CVP 6 hours postoperation was strongly associated with inhospital and 30-day mortality: odds ratio (OR) of 1.5 (95% confidence interval [CI], 1.23-1.87) for every 5-mm Hg increase in CVP; P<.0001. This association remained significant after risk adjustment: adjusted OR of 1.44 (95% CI, 1.10-1.89); P<.01. A model adjusting for cardiac index also revealed increased incidence of mortality or renal failure: adjusted OR of 1.5 (95% CI, 1.28-1.86) for every 5-mm Hg increase in CVP; P<.0001.
Conclusions: Patients' CVP at 6 hours after CABG surgery was highly predictive of operative mortality or renal failure, independent of cardiac index and other important clinical variables. Future studies will need to assess whether interventions guided by postoperative CVP can improve patient outcomes.
Keywords: Cardiac index; Central venous pressure; Coronary artery bypass; Hemodynamic monitoring; Perioperative care; Surgery.
Copyright © 2014 Elsevier Inc. All rights reserved.
Figures

References
-
- Schwann NM, Hillel Z, Hoeft A, Barash P, Mohnle P, Miao Y, Mangano DT. Lack of effectiveness of the pulmonary artery catheter in cardiac surgery. Anesth Analg. 2011;113:994–1002. - PubMed
-
- Shah MR, Hasselblad V, Stevenson LW, et al. Impact of the pulmonary artery catheter in critically ill patients: meta-analysis of randomized clinical trials. JAMA. 2005 Oct 5;294(13):1664–1670. - PubMed
-
- Welke KF, Ferguson TB, Coombs LP, Dokholyan RS, Murray CJ, Schrader MA, Peterson ED. Validity of the Society of Thoracic Surgeons National Adult Cardiac Surgery Database. Ann Thorac Surg. 2004;77:1137–1139. - PubMed
-
- Welke KF, Peterson ED, Vaughan-Sarrazin MS, O'Brien SM, Rosenthal GE, Shook GJ, Dokholyan RS, Haan CK, Ferguson TB., Jr Comparison of cardiac surgery volumes and mortality rates between the Society of Thoracic Surgeons and Medicare databases from 1993 through 2001. Ann Thorac Surg. 2007;84:1538–1546. - PubMed
-
- Shahian DM, Jacobs JP, Edwards FH, Brennan JM, Dokholyan RS, Prager RL, Wright CD, Peterson ED, McDonald DE, Grover FL. The Society of Thoracic Surgeons National Database. Heart. 2013 Jan 18; [Epub ahead of print] - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
