

Chronic stress, cortisol dysfunction, and pain: a psychoneuroendocrine rationale for stress management in pain rehabilitation
- PMID: 25035267
- PMCID: PMC4263906
- DOI: 10.2522/ptj.20130597
Chronic stress, cortisol dysfunction, and pain: a psychoneuroendocrine rationale for stress management in pain rehabilitation
Abstract
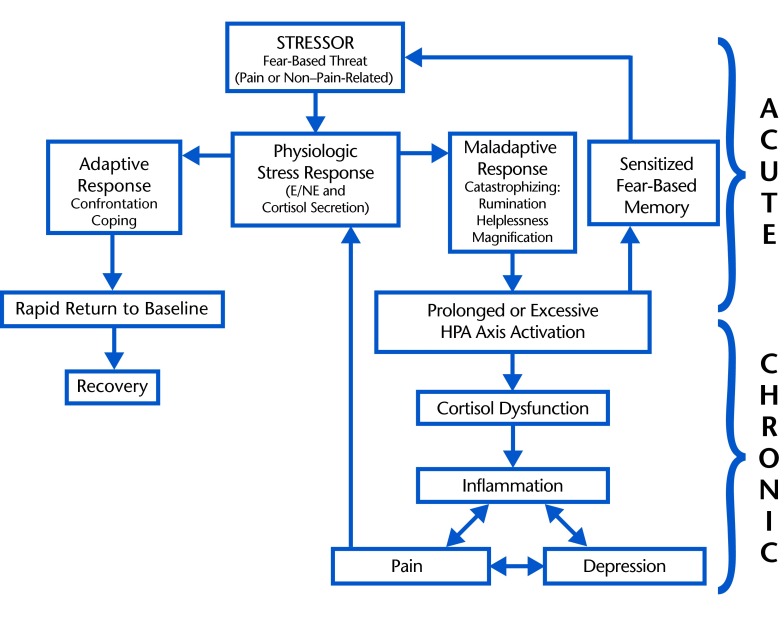
Pain is a primary symptom driving patients to seek physical therapy, and its attenuation commonly defines a successful outcome. A large body of evidence is dedicated to elucidating the relationship between chronic stress and pain; however, stress is rarely addressed in pain rehabilitation. A physiologic stress response may be evoked by fear or perceived threat to safety, status, or well-being and elicits the secretion of sympathetic catecholamines (epinephrine and norepinepherine) and neuroendocrine hormones (cortisol) to promote survival and motivate success. Cortisol is a potent anti-inflammatory that functions to mobilize glucose reserves for energy and modulate inflammation. Cortisol also may facilitate the consolidation of fear-based memories for future survival and avoidance of danger. Although short-term stress may be adaptive, maladaptive responses (eg, magnification, rumination, helplessness) to pain or non-pain-related stressors may intensify cortisol secretion and condition a sensitized physiologic stress response that is readily recruited. Ultimately, a prolonged or exaggerated stress response may perpetuate cortisol dysfunction, widespread inflammation, and pain. Stress may be unavoidable in life, and challenges are inherent to success; however, humans have the capability to modify what they perceive as stressful and how they respond to it. Exaggerated psychological responses (eg, catastrophizing) following maladaptive cognitive appraisals of potential stressors as threatening may exacerbate cortisol secretion and facilitate the consolidation of fear-based memories of pain or non-pain-related stressors; however, coping, cognitive reappraisal, or confrontation of stressors may minimize cortisol secretion and prevent chronic, recurrent pain. Given the parallel mechanisms underlying the physiologic effects of a maladaptive response to pain and non-pain-related stressors, physical therapists should consider screening for non-pain-related stress to facilitate treatment, prevent chronic disability, and improve quality of life.
© 2014 American Physical Therapy Association.
Figures
Comment in
-
On "chronic stress, cortisol dysfunction, and pain…" Hannibal KE, Bishop MD. Phys Ther. 2014;94:1816-1825.Phys Ther. 2015 Feb;95(2):274. doi: 10.2522/ptj.2015.95.2.274.1. Phys Ther. 2015. PMID: 25639527 No abstract available.
-
Author response.Phys Ther. 2015 Feb;95(2):274-5. doi: 10.2522/ptj.2015.95.2.274.2. Phys Ther. 2015. PMID: 25763431 No abstract available.
References
-
- Linton SJ. A review of psychological risk factors in back and neck pain. Spine (Phila Pa 1976). 2000;25:1148–1156. - PubMed
-
- Lucchetti G, Oliveira AB, Mercante JP, Peres MF. Anxiety and fear-avoidance in musculoskeletal pain. Curr Pain Headache Rep. 2012;16:399–406. - PubMed
-
- Ariëns GA, van Mechelen W, Bongers PM, et al. Psychosocial risk factors for neck pain: a systematic review. Am J Ind Med. 2001;39:180–193. - PubMed
-
- Main CJ, George SZ. Psychologically informed practice for management of low back pain: future directions in practice and research. Phys Ther. 2011;91:820–824. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
