

Facioscapulohumeral muscular dystrophy
- PMID: 25037087
- PMCID: PMC4239655
- DOI: 10.1016/j.ncl.2014.04.003
Facioscapulohumeral muscular dystrophy
Abstract
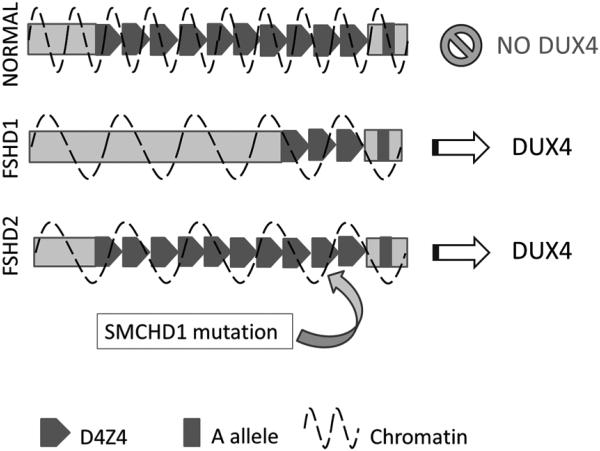
Facioscapulohumeral muscular dystrophy (FSHD) is a common type of adult muscular dystrophy and is divided into types 1 and 2 based on genetic mutation. Clinically, both FSHD types often show asymmetric and progressive muscle weakness affecting initially the face, shoulder, and arms followed by the distal then proximal lower extremities. Approximately 95% of patients, termed FSHD1, have a deletion of a key number of repetitive elements on chromosome 4q35. The remaining 5%, termed FSHD2, have no deletion on chromosome 4q35. Nevertheless, both types share a common downstream mechanism, making it possible for future disease-directed therapies to be effective for both FSHD types.
Keywords: D4Z4 deletion; DUX4; Facioscapulohumeral muscular dystrophy; Muscular dystrophy; SMCHD1 mutation.
Copyright © 2014 Elsevier Inc. All rights reserved.
Figures
References
-
- Mostacciuolo ML, Pastorello E, Vazza G, et al. Facioscapulohumeral muscular dystrophy: epidemiological and molecular study in a north-east Italian population sample. Clin Genet. 2009;75(6):550–555. - PubMed
-
- Padberg GW, Frants RR, Brouwer OF, et al. Facioscapulohumeral muscular dystrophy in the Dutch population. Muscle Nerve. 1995;2:S81–84. - PubMed
-
- van Deutekom JC, Wijmenga C, van Tienhoven EA, et al. FSHD associated DNA rearrangements are due to deletions of integral copies of a 3.2 kb tandemly repeated unit. Hum Mol Genet. 1993;2(12):2037–2042. - PubMed
-
- Wijmenga C, Hewitt JE, Sandkuijl LA, et al. Chromosome 4q DNA rearrangements associated with facioscapulohumeral muscular dystrophy. Nat Genet. 1992;2(1):26–30. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
