

Assessment of dyspnea early in acute heart failure: patient characteristics and response differences between likert and visual analog scales
- PMID: 25039550
- PMCID: PMC4105984
- DOI: 10.1111/acem.12390
Assessment of dyspnea early in acute heart failure: patient characteristics and response differences between likert and visual analog scales
Abstract
Background: Dyspnea is the most common symptom in acute heart failure (AHF), yet how to best measure it has not been well defined. Prior studies demonstrate differences in dyspnea improvement across various measurement scales, yet these studies typically enroll patients well after the emergency department (ED) phase of management.
Objectives: The aim of this study was to determine predictors of early dyspnea improvement for three different, commonly used dyspnea scales (i.e., five-point absolute Likert scale, 10-cm visual analog scale [VAS], or seven-point relative Likert scale).
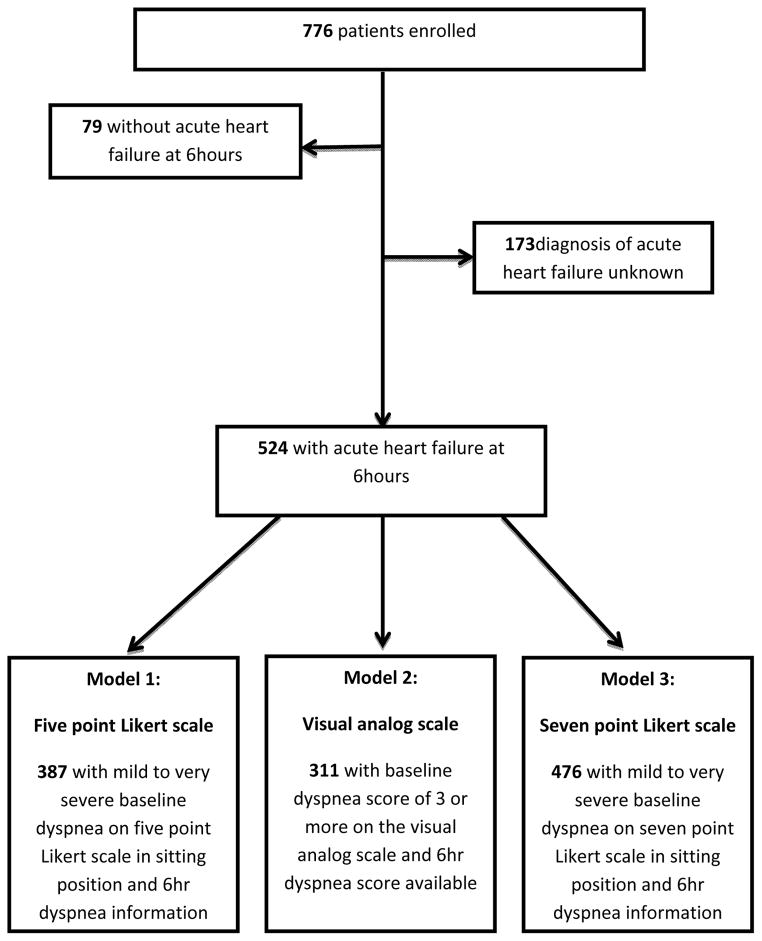
Methods: This was a post hoc analysis of URGENT Dyspnea, an observational study of 776 patients in 17 countries enrolled within 1 hour of first physician encounter. Inclusion criteria were broad to reflect real-world clinical practice. Prior literature informed the a priori definition of clinically significant dyspnea improvement. Resampling-based multivariable models were created to determine patient characteristics significantly associated with dyspnea improvement.
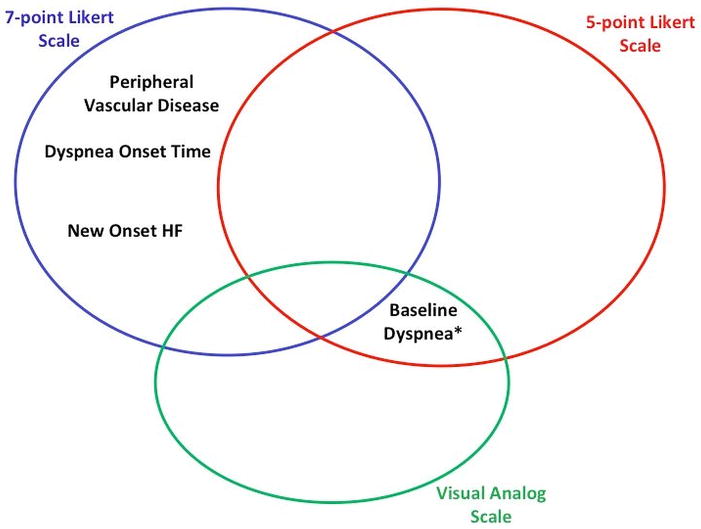
Results: Of the 524 AHF patients, approximately 40% of patients did not report substantial dyspnea improvement within the first 6 hours. Baseline characteristics were similar between those who did or did not improve, although there were differences in history of heart failure, coronary artery disease, and initial systolic blood pressure. For those who did improve, patient characteristics differed across all three scales, with the exception of baseline dyspnea severity for the VAS and five-point Likert scale (c-index ranged from 0.708 to 0.831 for each scale).
Conclusions: Predictors of early dyspnea improvement differ from scale to scale, with the exception of baseline dyspnea. Attempts to use one scale to capture the entirety of the dyspnea symptom may be insufficient.
© 2014 by the Society for Academic Emergency Medicine.
Figures
References
-
- Yancy CW, Lopatin M, Stevenson LW, De Marco T, Fonarow GC. Clinical presentation, management, and in-hospital outcomes of patients admitted with acute decompensated heart failure with preserved systolic function: a report from the Acute Decompensated Heart Failure National Registry (ADHERE) database. J Am Coll Cardiol. 2006;47:76–84. - PubMed
-
- Abraham WT, Adams KF, Fonarow GC, et al. In-hospital mortality in patients with acute decompensated heart failure requiring intravenous vasoactive medications: an analysis from the Acute Decompensated Heart Failure National Registry (ADHERE) J Am Coll Cardiol. 2005;46:57–64. - PubMed
-
- Metra M, Cleland JG, Weatherley BD, et al. Dyspnoea in patients with acute heart failure: an analysis of its clinical course, determinants, and relationship to 60-day outcomes in the PROTECT pilot study. Eur J Heart Fail. 2010;12:499–507. - PubMed
-
- Metra M, O’Connor CM, Davison BA, et al. Early dyspnoea relief in acute heart failure: prevalence, association with mortality, and effect of rolofylline in the PROTECT Study. Eur Heart J. 2011;32:1519–34. - PubMed
-
- Pang PS, Cleland JG, Teerlink JR, et al. A proposal to standardize dyspnoea measurement in clinical trials of acute heart failure syndromes: the need for a uniform approach. Eur Heart J. 2008;29:816–24. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
