

Association of low numbers of CD206-positive cells with loss of ICC in the gastric body of patients with diabetic gastroparesis
- PMID: 25041465
- PMCID: PMC4149814
- DOI: 10.1111/nmo.12389
Association of low numbers of CD206-positive cells with loss of ICC in the gastric body of patients with diabetic gastroparesis
Abstract
Background: There is increasing evidence for specific cellular changes in the stomach of patients with diabetic (DG) and idiopathic (IG) gastroparesis. The most significant findings are loss of interstitial cells of Cajal (ICC), neuronal abnormalities, and an immune cellular infiltrate. Studies done in diabetic mice have shown a cytoprotective effect of CD206+ M2 macrophages. To quantify overall immune cellular infiltrate, identify macrophage populations, and quantify CD206+ and iNOS+ cells. To investigate associations between cellular phenotypes and ICC.
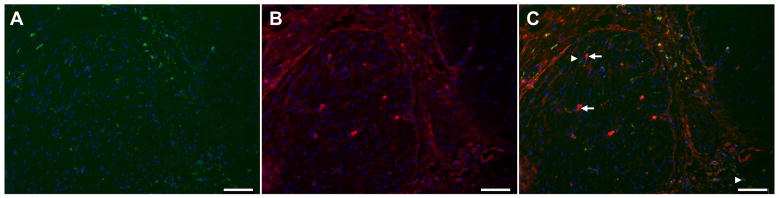
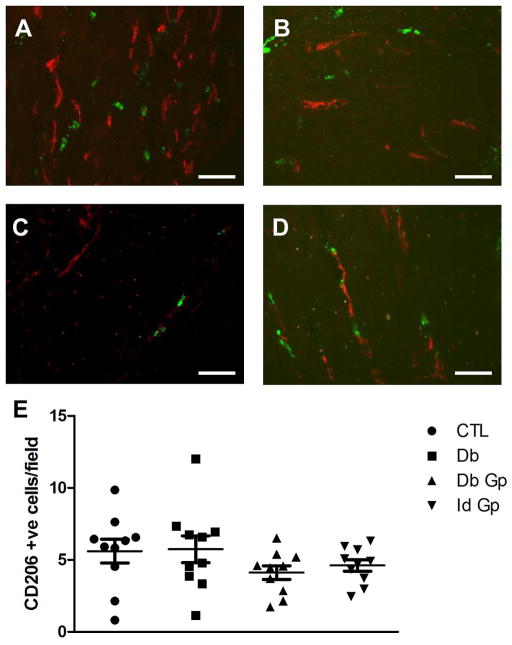
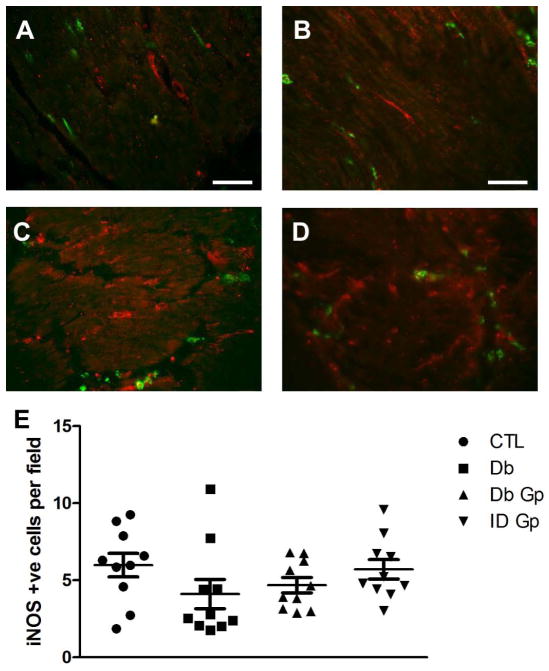
Methods: Full thickness gastric body biopsies were obtained from non-diabetic controls (C), diabetic controls (DC), DG, and IG patients. Sections were labeled for CD45, CD206, Kit, iNOS, and putative human macrophage markers (HAM56, CD68, and EMR1). Immunoreactive cells were quantified from the circular muscle layer.
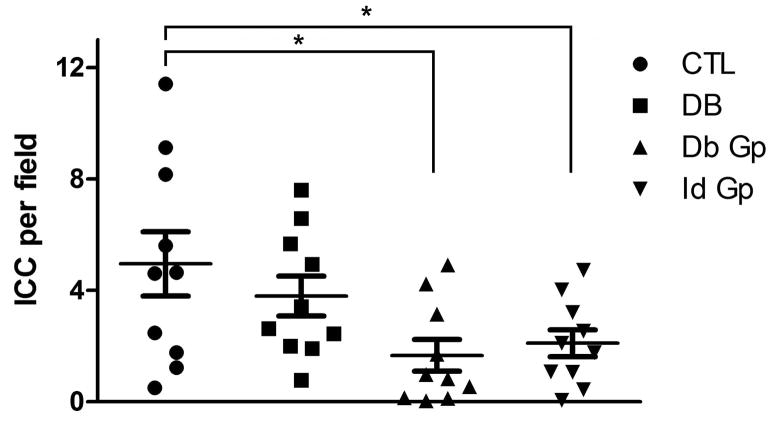
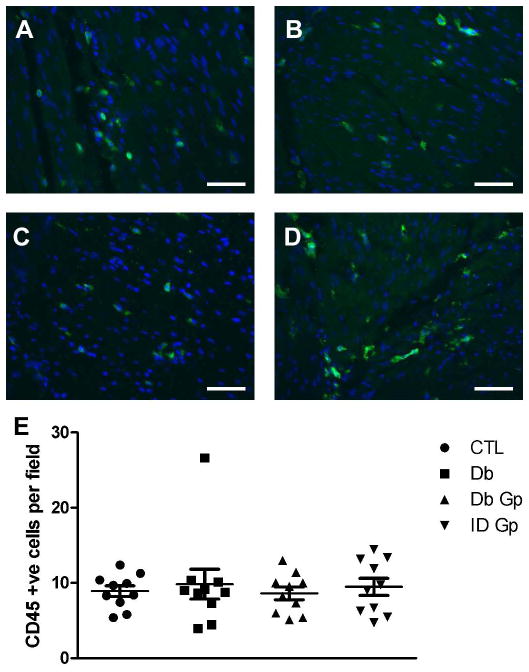
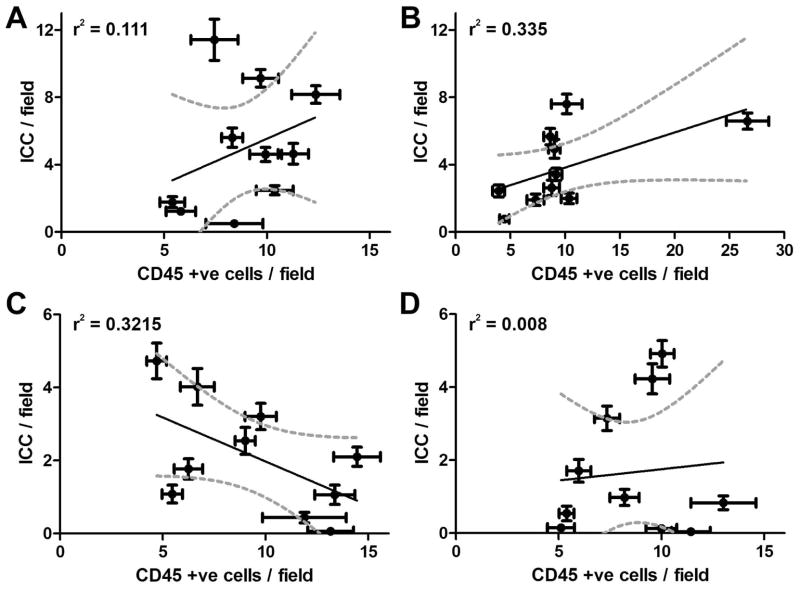
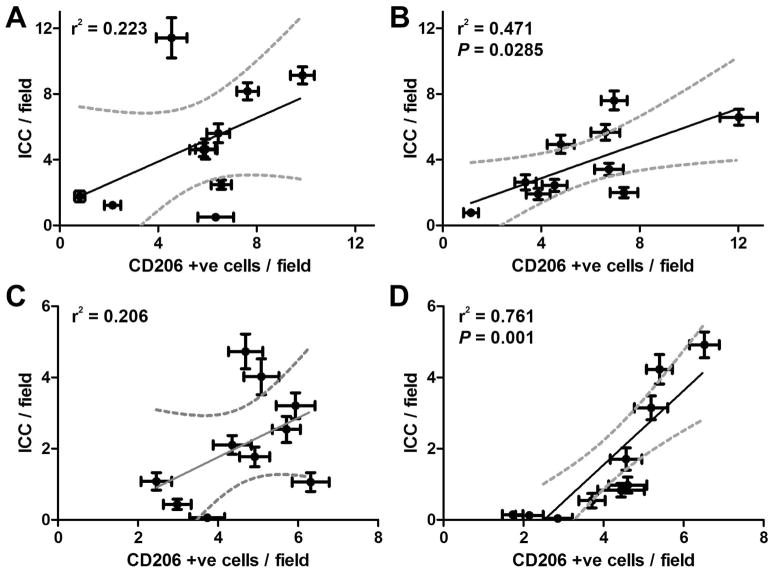
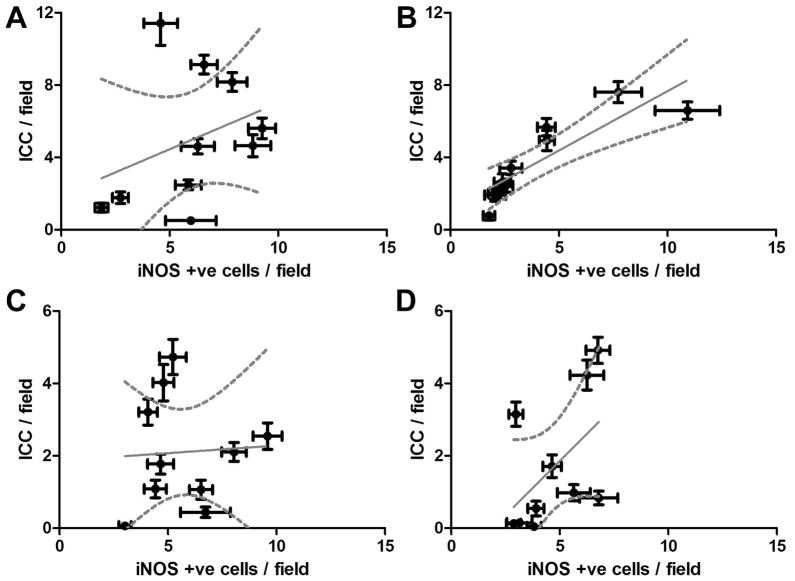
Key results: Significantly fewer ICC were detected in DG and IG tissues, but there were no differences in the numbers of cells immunoreactive for other markers between patient groups. There was a significant correlation between the number of CD206+ cells and ICC in DG and DC patients, but not in C and IG and a significant correlation between iNOS+ cells and ICC in the DC group, but not the other groups. CD68 and HAM56 reliably labeled the same cell populations, but EMR1 labeled other cell types.
Conclusions & inferences: Depletion of ICC and correlation with changes in CD206+ cell numbers in DC and DG patients suggests that in humans, like mice, CD206+ macrophages may play a cytoprotective role in diabetes. These findings may lead to novel therapeutic options, targeting alternatively activated macrophages.
Keywords: gastroparesis; interstitial cells of Cajal; macrophages.
© 2014 John Wiley & Sons Ltd.
Figures
References
-
- Wang YR, Fisher RS, Parkman HP. Gastroparesis-related hospitalizations in the United States: trends, characteristics, and outcomes, 1995–2004. Am J Gastroenterol. 2008;103:313–22. - PubMed
-
- Parkman HP, Hasler WL, Fisher RS. American Gastroenterological Association technical review on the diagnosis and treatment of gastroparesis. Gastroenterology. 2004;127:1592–622. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 DK074008/DK/NIDDK NIH HHS/United States
- UL1TR000135/TR/NCATS NIH HHS/United States
- UL1TR000093/TR/NCATS NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- UL1 TR000093/TR/NCATS NIH HHS/United States
- U01 DK073985/DK/NIDDK NIH HHS/United States
- U01 DK073975/DK/NIDDK NIH HHS/United States
- U01 DK074035/DK/NIDDK NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- U01DK074008/DK/NIDDK NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- U01DK073983/DK/NIDDK NIH HHS/United States
- U01DK073985/DK/NIDDK NIH HHS/United States
- UL1TR000424/TR/NCATS NIH HHS/United States
- U01DK073974/DK/NIDDK NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- U01DK073975/DK/NIDDK NIH HHS/United States
- UL1TR000433/TR/NCATS NIH HHS/United States
- R01 DK057061/DK/NIDDK NIH HHS/United States
- P01 DK068055/DK/NIDDK NIH HHS/United States
- U01 DK074007/DK/NIDDK NIH HHS/United States
- U01 DK073983/DK/NIDDK NIH HHS/United States
- UL1 TR000135/TR/NCATS NIH HHS/United States
- U01DK074035/DK/NIDDK NIH HHS/United States
- U01DK074007/DK/NIDDK NIH HHS/United States
- UL1 TR001085/TR/NCATS NIH HHS/United States
- U01 DK073974/DK/NIDDK NIH HHS/United States
- P30 DK084567/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
