

Dual blockade of epidermal growth factor receptor and insulin-like growth factor receptor-1 signaling in metastatic pancreatic cancer: phase Ib and randomized phase II trial of gemcitabine, erlotinib, and cixutumumab versus gemcitabine plus erlotinib (SWOG S0727)
- PMID: 25041791
- PMCID: PMC4284963
- DOI: 10.1002/cncr.28744
Dual blockade of epidermal growth factor receptor and insulin-like growth factor receptor-1 signaling in metastatic pancreatic cancer: phase Ib and randomized phase II trial of gemcitabine, erlotinib, and cixutumumab versus gemcitabine plus erlotinib (SWOG S0727)
Abstract
Background: Targeting a single pathway in pancreatic adenocarcinoma (PC) is unlikely to affect its natural history. We tested the hypothesis that simulataneous targeting of the epidermal growth factor receptor (EGFR) and insulin-like growth factor receptor-1 (IGF-1R) pathways would significantly improve progression-free survival (PFS) by abrogating reciprocal signaling that promote drug resistance
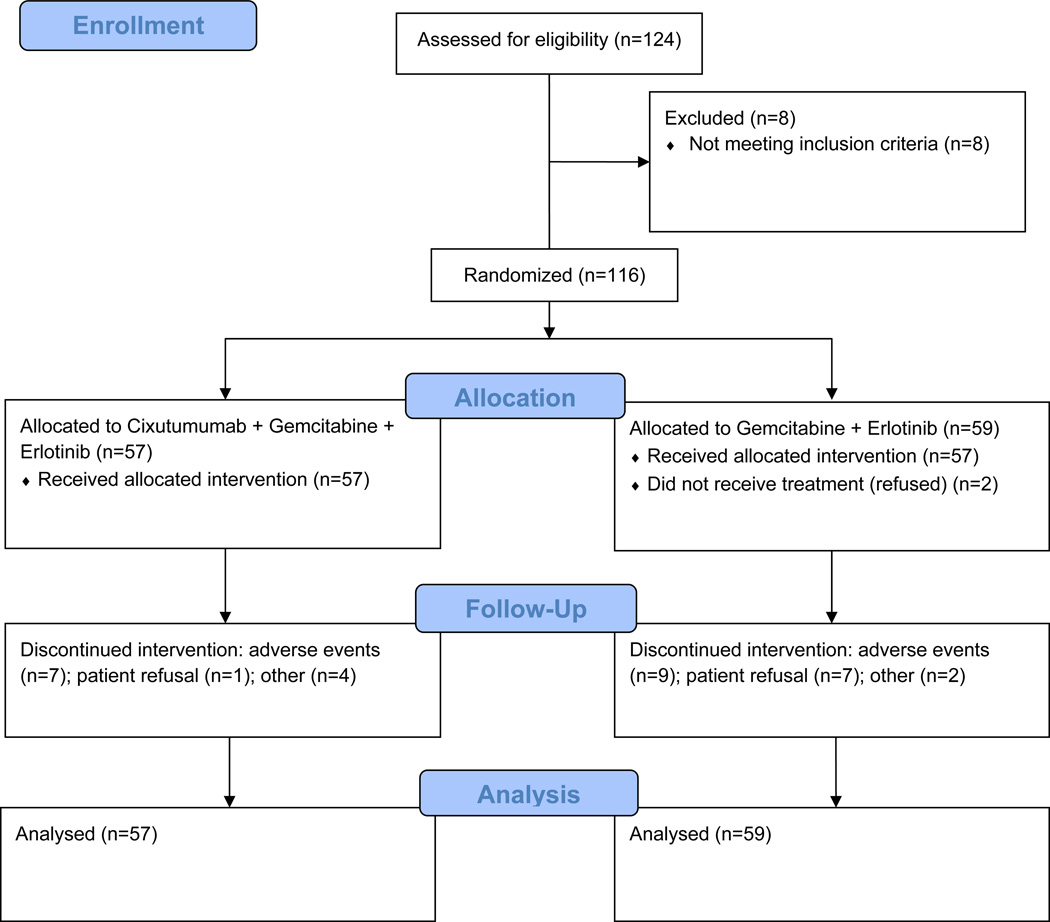
Methods: This was a phase Ib/II study testing cixutumumab, combined with erlotinib and gemcitabine (G) in patients with untreated metastatic PC. The control arm was erlotinib plus G. The primary end point was PFS. Eligibility included performance status 0/1 and normal fasting blood glucose. Polymorphisms in genes involved in G metabolism and in the EGFR pathway were also studied
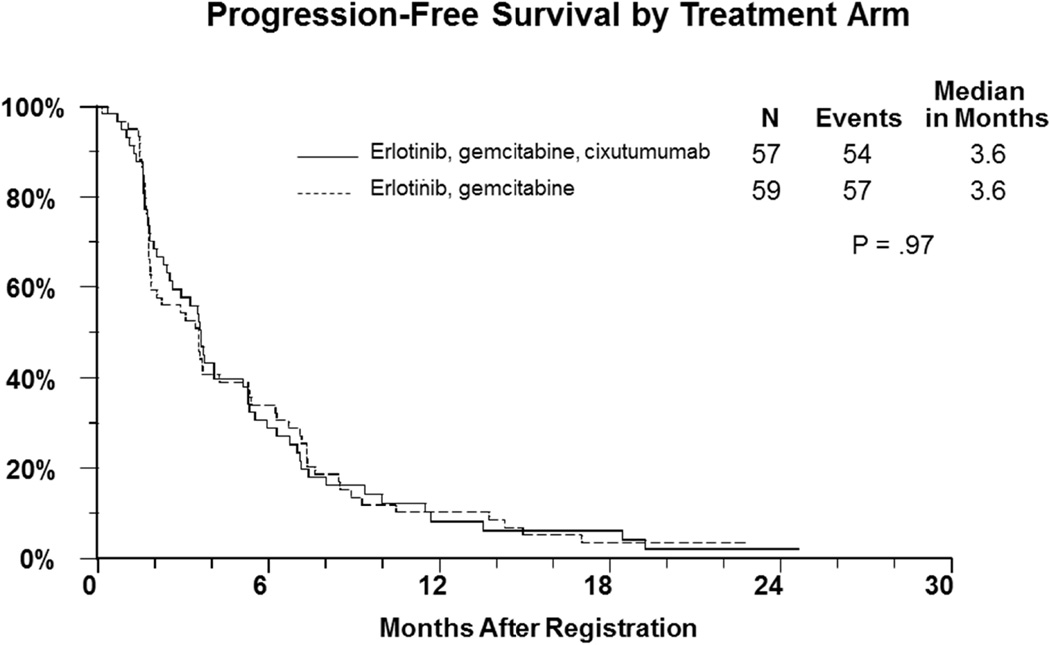
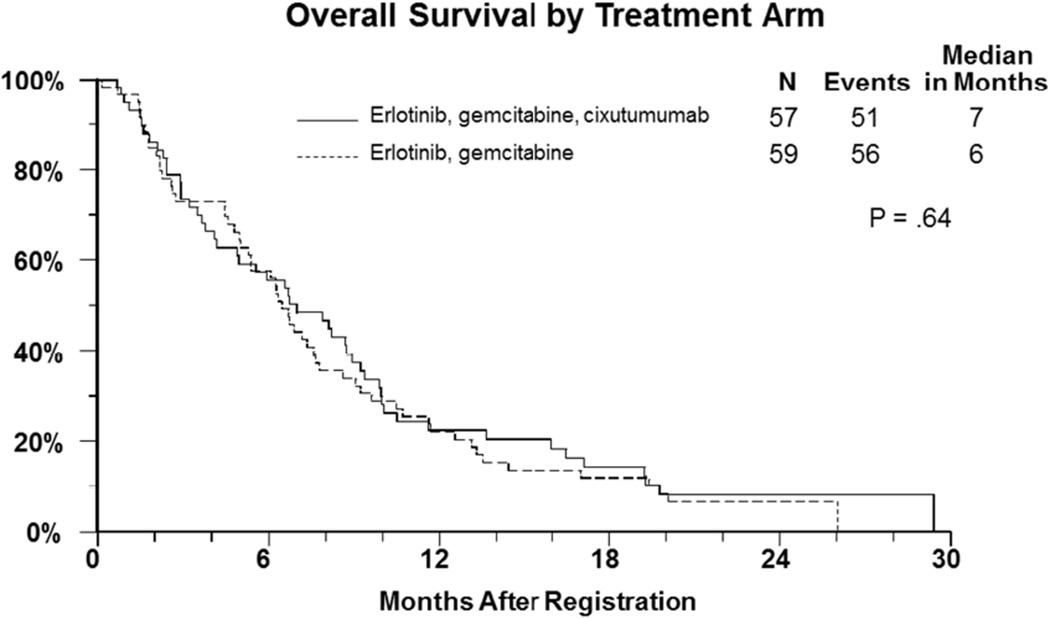
Results: The phase I results (n = 10) established the safety of cixutumumab 6 mg/kg/week intravenously, erlotinib 100 mg/day orally, and G 1000 mg/m(2) intravenously on days 1, 8, and 15 of a 28-day cycle. In the RP2 portion (116 eligible patients; median age, 63), the median PFS and overall survival (OS) were 3.6 and 7.0 months, respectively, on the cixutumumab arm, and 3.6 and 6.7 months, respecively, on the control arm. Major grades 3 and 4 toxicities with cixutumumab and control were elevation of transaminases, 12% and 6%, respectively; fatigue, 16% and 12%, respectively; gastrointestinal, 35% and 28%, respectively; neutropenia, 21% and 10%, respectively; and thrombocytopenia, 16% and 7%, respecively. Grade 3/4 hyperglycemia was seen in 16% of patients on cixutumumab. Grade 3 or 4 skin toxicity was similar in both arms of the study (< 5%). No significant differences in PFS by genotype were seen for any of the polymorphisms.
Conclusions: Adding the IGF-1R inhibitor cixutumumab to erlotinib and G did not lead to longer PFS or OS in metastatic PC.
Keywords: EGFR; IGF-1R; cixutumumab; erlotinib signaling; pancreatic cancer; randomized phase II; targeted treatment.
© 2014 American Cancer Society.
Conflict of interest statement
Figures
References
-
- Siegel R, Ward E, Brawley O, Jemal A. Cancer statistics, 2011: the impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J Clin. 2011;61(4):212–236. - PubMed
-
- Philip PA. Novel targets for pancreatic cancer therapy. Surg Oncol Clin N Am. 2010;19(2):419–429. - PubMed
-
- Rieder S, Michalski CW, Friess H, Kleeff J. Insulin-like growth factor signaling as a therapeutic target in pancreatic cancer. Anticancer Agents Med Chem. 2011;11(5):427–433. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- CA76462/CA/NCI NIH HHS/United States
- U10 CA045808/CA/NCI NIH HHS/United States
- CA58861/CA/NCI NIH HHS/United States
- U10 CA035178/CA/NCI NIH HHS/United States
- U10 CA042777/CA/NCI NIH HHS/United States
- CA58723/CA/NCI NIH HHS/United States
- CA86780/CA/NCI NIH HHS/United States
- CA37981/CA/NCI NIH HHS/United States
- U10 CA022433/CA/NCI NIH HHS/United States
- U10 CA027057/CA/NCI NIH HHS/United States
- N01 CA035176/CA/NCI NIH HHS/United States
- CA139519/CA/NCI NIH HHS/United States
- U10 CA037981/CA/NCI NIH HHS/United States
- CA22433/CA/NCI NIH HHS/United States
- CA073590/CA/NCI NIH HHS/United States
- U10 CA046113/CA/NCI NIH HHS/United States
- CA20319/CA/NCI NIH HHS/United States
- U10 CA076447/CA/NCI NIH HHS/United States
- U10 CA128567/CA/NCI NIH HHS/United States
- N01 CA032102/CA/NCI NIH HHS/United States
- N01 CA045807/CA/NCI NIH HHS/United States
- CA128567/CA/NCI NIH HHS/United States
- U10 CA014028/CA/NCI NIH HHS/United States
- CA45808/CA/NCI NIH HHS/United States
- N01 CA046441/CA/NCI NIH HHS/United States
- U10 CA139519/CA/NCI NIH HHS/United States
- CA14028/CA/NCI NIH HHS/United States
- CA58882/CA/NCI NIH HHS/United States
- U10 CA074647/CA/NCI NIH HHS/United States
- CA11083/CA/NCI NIH HHS/United States
- U10 CA045461/CA/NCI NIH HHS/United States
- CA76447/CA/NCI NIH HHS/United States
- U10 CA045450/CA/NCI NIH HHS/United States
- U10 CA032102/CA/NCI NIH HHS/United States
- CA45450/CA/NCI NIH HHS/United States
- CA46368/CA/NCI NIH HHS/United States
- N01 CA035178/CA/NCI NIH HHS/United States
- N01 CA038926/CA/NCI NIH HHS/United States
- U10 CA067575/CA/NCI NIH HHS/United States
- P30 CA022453/CA/NCI NIH HHS/United States
- N01 CA027057/CA/NCI NIH HHS/United States
- U10 CA073590/CA/NCI NIH HHS/United States
- U10 CA046441/CA/NCI NIH HHS/United States
- U10 CA058882/CA/NCI NIH HHS/United States
- CA74647/CA/NCI NIH HHS/United States
- U10 CA020319/CA/NCI NIH HHS/United States
- CA46113/CA/NCI NIH HHS/United States
- U10 CA038926/CA/NCI NIH HHS/United States
- CA76448/CA/NCI NIH HHS/United States
- U10 CA086780/CA/NCI NIH HHS/United States
- U10 CA095860/CA/NCI NIH HHS/United States
- CA42777/CA/NCI NIH HHS/United States
- CA52654/CA/NCI NIH HHS/United States
- U10 CA046368/CA/NCI NIH HHS/United States
- CA4461/CA/NCI NIH HHS/United States
- N01 CA067575/CA/NCI NIH HHS/United States
- U10 CA052654/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- U10 CA180819/CA/NCI NIH HHS/United States
- U10 CA035176/CA/NCI NIH HHS/United States
- CA95860/CA/NCI NIH HHS/United States
- U10 CA058861/CA/NCI NIH HHS/United States
- U10 CA045807/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
