

CXCR5+ CD4+ T follicular helper cells participate in the pathogenesis of primary biliary cirrhosis
- PMID: 25042122
- PMCID: PMC4507804
- DOI: 10.1002/hep.27306
CXCR5+ CD4+ T follicular helper cells participate in the pathogenesis of primary biliary cirrhosis
Abstract
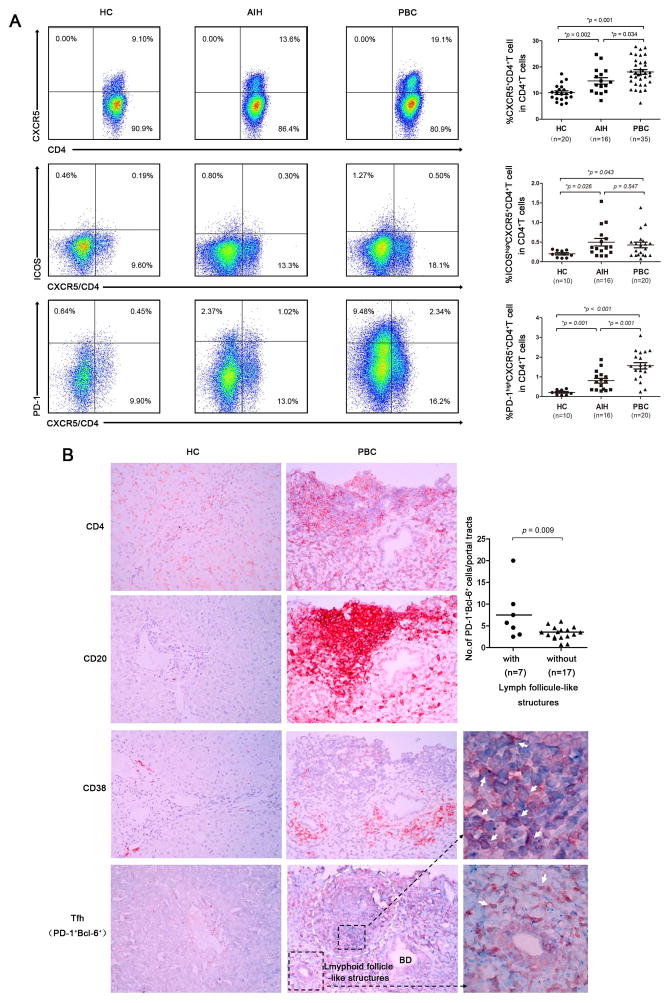
There is increasing interest in the role of T follicular helper (Tfh) cells in autoimmunity from the perspective of both their role in breach of tolerance and their effects on the natural history of disease progression. Indeed, the critical role of Tfh cells in autoimmunity is further highlighted based on their location in the germinal center (GC), a pathogenic hot spot for development of autoreactivity. To address the role of Tfh cells in primary biliary cirrhosis (PBC), we comprehensively evaluated the immunobiology of CXCR5(+) CD4(+) Tfh cells in 69 patients with PBC, including a nested subgroup of 16 autoimmune hepatitis (AIH) and 20 healthy controls (HC), followed for 1 year. We report herein several key observations. First, there was an increased frequency of circulating Tfh cells in patients with PBC compared to AIH (P < 0.05) and HC (P < 0.01). Second, the function of circulating Tfh cells from PBC patients, including interleukin (IL)-21 production (P < 0.05), the ability to promote B-cell maturation, and autoantibody production, were greater than HC. Third, the frequency of these cells was significantly decreased in ursodeoxycholic acid (UDCA) responders compared to UDCA-treated nonresponders, in both cross-sectional (P = 0.023) and longitudinal studies (P = 0.036), respectively. Indeed, similar increases of Tfh cells were noted in liver and spleen.
Conclusion: These results significantly extend our understanding of lymphoid subpopulations in PBC and their relative role in disease expression. Our data also provide a novel biomarker for evaluation of the effectiveness of new therapeutic approaches.
© 2014 by the American Association for the Study of Liver Diseases.
Figures




Comment in
-
Follicles, germinal centers, and immune mechanisms in primary biliary cirrhosis.Hepatology. 2015 Feb;61(2):424-7. doi: 10.1002/hep.27552. Hepatology. 2015. PMID: 25294750 No abstract available.
References
-
- Kaplan MM, Gershwin ME. Primary biliary cirrhosis. N Engl J Med. 2005;353:1261–1273. - PubMed
-
- Selmi C, Bowlus CL, Gershwin ME, Coppel RL. Primary biliary cirrhosis. Lancet. 2011;377:1600–1609. - PubMed
-
- Kita H, Lian ZX, Van de Water J, He XS, Matsumura S, Kaplan M, Luketic V, et al. Identification of HLA-A2-restricted CD8(+) cytotoxic T cell responses in primary biliary cirrhosis: T cell activation is augmented by immune complexes cross-presented by dendritic cells. J Exp Med. 2002;195:113–123. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous