

Genetic and phenotypic diversity of NHE6 mutations in Christianson syndrome
- PMID: 25044251
- PMCID: PMC4304796
- DOI: 10.1002/ana.24225
Genetic and phenotypic diversity of NHE6 mutations in Christianson syndrome
Abstract
Objective: Recently, Christianson syndrome (CS) has been determined to be caused by mutations in the X-linked Na(+) /H(+) exchanger 6 (NHE6). We aimed to determine the diagnostic criteria and mutational spectrum for CS.
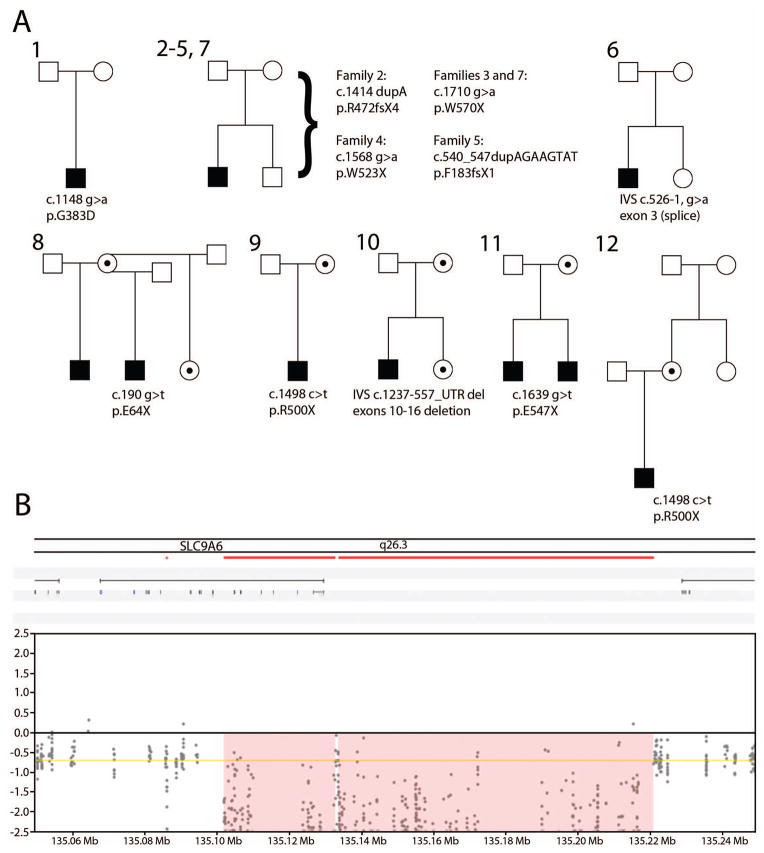
Methods: Twelve independent pedigrees (14 boys, age = 4-19 years) with mutations in NHE6 were administered standardized research assessments, and mutations were characterized.
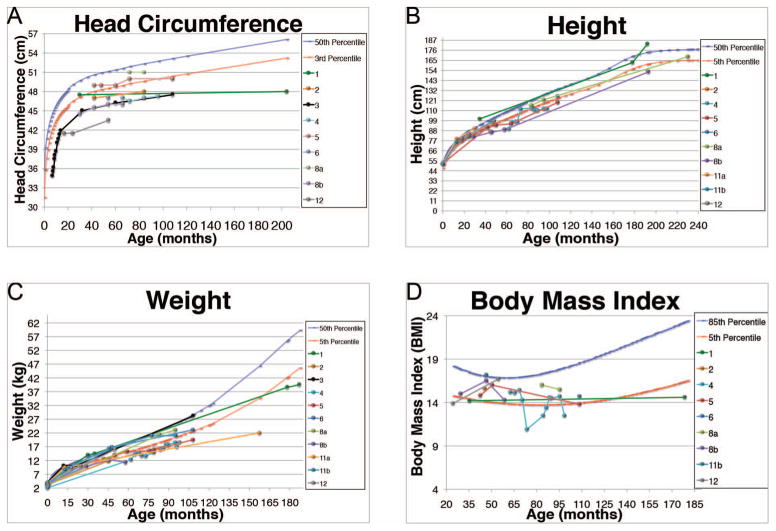
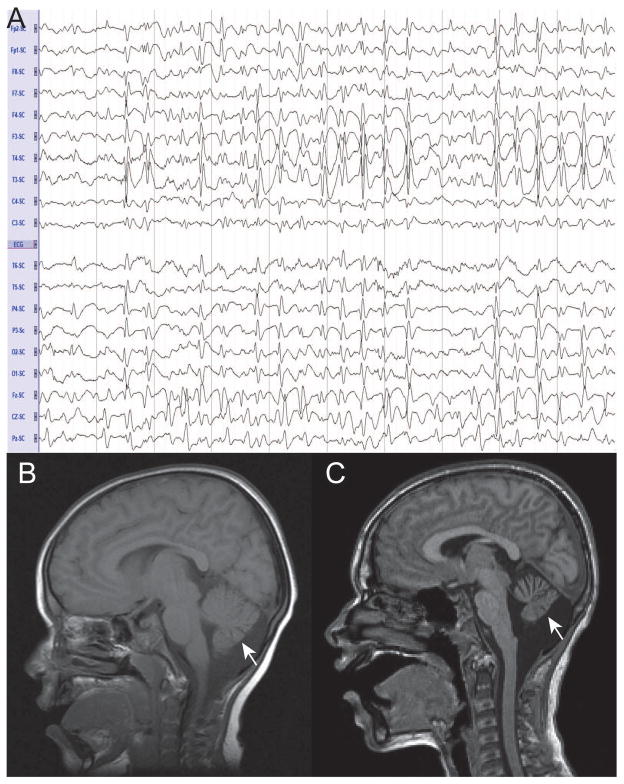
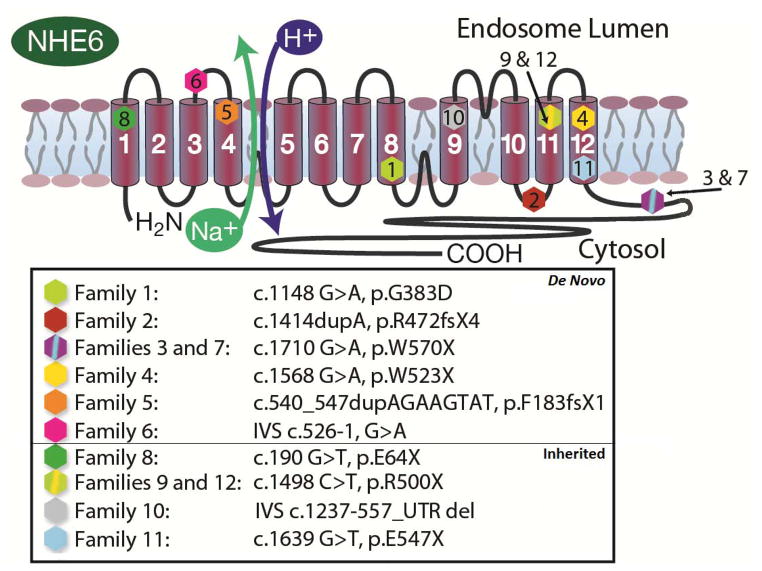
Results: The mutational spectrum was composed of 9 single nucleotide variants, 2 indels, and 1 copy number variation deletion. All mutations were protein-truncating or splicing mutations. We identified 2 recurrent mutations (c.1498 c>t, p.R500X; and c.1710 g>a, p.W570X). Otherwise, all mutations were unique. In our study, 7 of 12 mutations (58%) were de novo, in contrast to prior literature wherein mutations were largely inherited. We also report prominent neurological, medical, and behavioral symptoms. All CS participants were nonverbal and had intellectual disability, epilepsy, and ataxia. Many had prior diagnoses of autism and/or Angelman syndrome. Other neurologic symptoms included eye movement abnormalities (79%), postnatal microcephaly (92%), and magnetic resonance imaging evidence of cerebellar atrophy (33%). Regression was noted in 50%, with recurrent presentations involving loss of words and/or the ability to walk. Medical symptoms, particularly gastrointestinal symptoms, were common. Height and body mass index measures were below normal ranges in most participants. Behavioral symptoms included hyperkinetic behavior (100%), and a majority exhibited high pain threshold.
Interpretation: This is the largest cohort of independent CS pedigrees reported. We propose diagnostic criteria for CS. CS represents a novel neurogenetic disorder with general relevance to autism, intellectual disability, Angelman syndrome, epilepsy, and regression.
© 2014 American Neurological Association.
Conflict of interest statement
None of the authors have a financial conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
