

Use of percutaneous image-guided coaxial core-needle biopsy for diagnosis of intraabdominal lymphoma
- PMID: 25044810
- PMCID: PMC4302683
- DOI: 10.1002/cam4.224
Use of percutaneous image-guided coaxial core-needle biopsy for diagnosis of intraabdominal lymphoma
Abstract
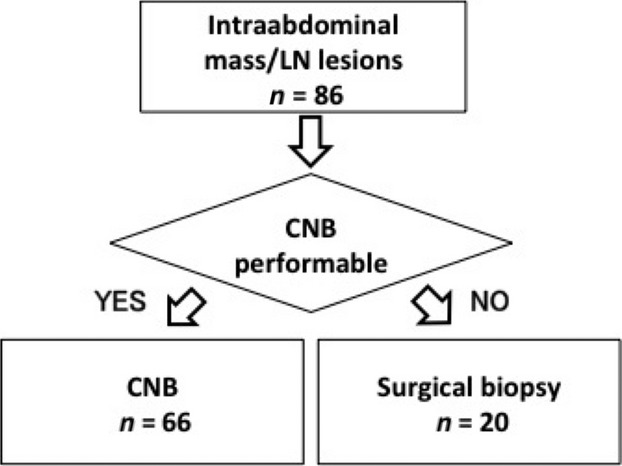
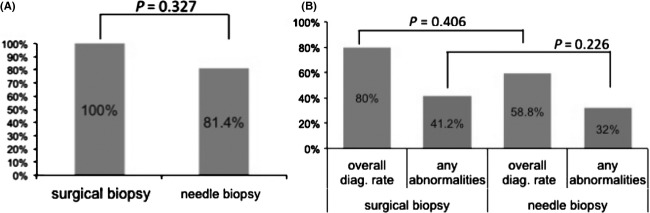
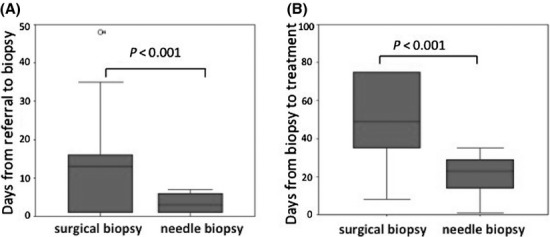
Although pathological diagnosis is essential for managing malignant lymphoma, intraabdominal lesions are generally difficult to approach due to the invasiveness of abdominal surgery. Here, we report the use of percutaneous image-guided coaxial core-needle biopsy (CNB) to obtain intraabdominal specimens for diagnosing intraabdominal lymphomas, which typically requires histopathological and immunohistochemical evaluation. We retrospectively reviewed consecutive cases involving computed tomography (CT)- or ultrasonography (US)-guided CNB to obtain pathological specimens for intraabdominal lesions from 1999 to 2011. Liver, spleen, kidney, and inguinal node biopsies were excluded. We compared CNBs with laparotomic biopsies. A total of 66 CNBs were performed for 59 patients (32 males, 27 females; median age, 63.5), including second or third repeat procedures. Overall diagnostic rate was 88.5%. None of the patients required additional surgical biopsies. Notably, the median interval between recognition of an intraabdominal mass and biopsy was only 1 day. Forty-five procedures were performed for hematological malignancies. Adequate specimens were obtained for histopathological diagnosis in 86% of cases. Flow cytometry detected lymphoma cells in 79.5% of cases. Twelve patients (nine males, three females; median age, 60) were eligible for surgical biopsy. While every postoperative course was satisfactory, median duration from lesion recognition to therapy initiation for lymphoma cases was significantly shorter for CNB than for surgical biopsy (14 vs. 35 days). While one-fourth of the patients were not eligible for the procedures, CNB is safe and highly effective for diagnosis of intraabdominal lymphomas. This method significantly improves sampling and potentially helps attain immunohistological distinction, allowing for more timely therapy initiation.
Keywords: Diagnosis; immunophenotype; malignant lymphoma; needle biopsy; sensitivity and specificity.
© 2014 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Figures
References
-
- Kadin ME, Berard CW, Nanba K, Wakasa H. Lymphoproliferative diseases in Japan and Western countries: Proceedings of the United States-Japan Seminar, September 6 and 7, 1982, in Seattle. Washington. Hum. Pathol. 1983;14:745–772. - PubMed
-
- Jaffe ES, Harris NL, Stein H, Campo H, Pileri SA. Introduction and overview of the classification of the lymphoid neoplasms. In: Werdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW, Swerdlow SH, editors. WHO classification of tumours of haematopoietic and lymphoid tissues. 4th ed. Lyon, France: IARC; 2008. pp. 158–166.
-
- Takahashi H, Tomita N, Yokoyama M, Tsunoda S, Yano T, Murayama K, et al. Prognostic impact of extranodal involvement in diffuse large B-cell lymphoma in the rituximab era. Cancer. 2012;118:4166–4172. - PubMed
-
- Zornoza J, Cabanillas FF, Altoff TM, Ordonez N, Cohen MA. Percutaneous needle biopsy in abdominal lymphoma. AJR Am. J. Roentgenol. 1981;136:97–103. - PubMed
-
- Kälkner M, Rehn S, Andersson T, Elvin A, Hagberg H, Lindgren PG, et al. Diagnostics of malignant lymphomas with ultrasound guided 1.2 mm biopsy-gun. Acta Oncol. 1994;33:33–37. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
