

UTE imaging in the musculoskeletal system
- PMID: 25045018
- PMCID: PMC4297256
- DOI: 10.1002/jmri.24713
UTE imaging in the musculoskeletal system
Abstract
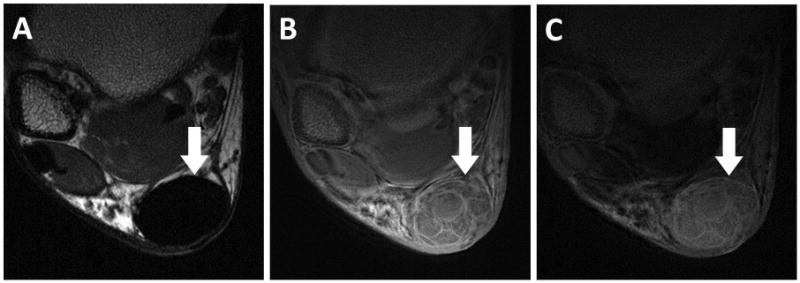
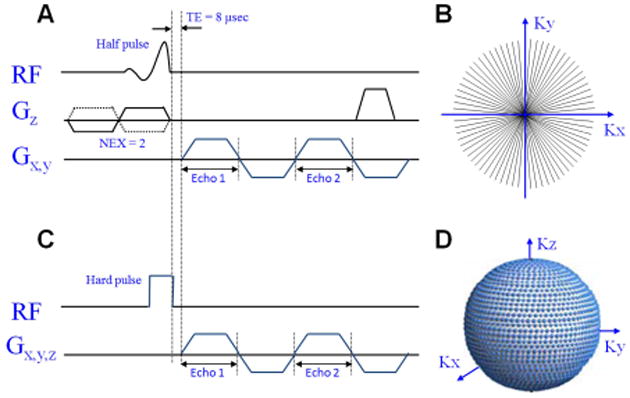
Tissues, such as bone, tendon, and ligaments, contain a high fraction of components with "short" and "ultrashort" transverse relaxation times and therefore have short mean transverse relaxation times. With conventional magnetic resonance imaging (MRI) sequences that employ relatively long echo times (TEs), there is no opportunity to encode the decaying signal of short and ultrashort T2 /T2 * tissues before it has reached zero or near zero. The clinically compatible ultrashort TE (UTE) sequence has been increasingly used to study the musculoskeletal system. This article reviews the UTE sequence as well as various modifications that have been implemented since its introduction. These modifications have been used to improve efficiency or contrast as well as provide quantitative analysis. This article reviews several clinical musculoskeletal applications of UTE.
Keywords: bicomponent analysis; musculoskeletal tissues; quantitative MRI; ultrashort TE.
© 2014 Wiley Periodicals, Inc.
Figures
References
-
- Pauly JM, Conolly SI, Nishimura D, Macovski A. Slice-Selective Excitation for Very Short T2 Species. Proceedings of the 8th Annual Meeting of ISMRM; Amsterdamn, Netherlands. 1989; abstract 28.
-
- Du J, Carl M, Diaz E, et al. Ultrashort TE T1rho (UTE T1rho) imaging of the Achilles tendon and meniscus. Magn Reson Med. 2010;64(3):834–842. - PubMed
-
- Rahmer J, Bornert P, Groen J, Bos C. Three-dimensional radial ultrashort echo-time imaging with T2 adapted sampling. Magn Reson Med. 2006;55(5):1075–1082. - PubMed
-
- Pauly JM. Selective Excitation for Ultrashort Echo Time Imaging. eMagRes: John Wiley & Sons, Ltd; 2012. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
