

Actinomycosis: etiology, clinical features, diagnosis, treatment, and management
- PMID: 25045274
- PMCID: PMC4094581
- DOI: 10.2147/IDR.S39601
Actinomycosis: etiology, clinical features, diagnosis, treatment, and management
Abstract
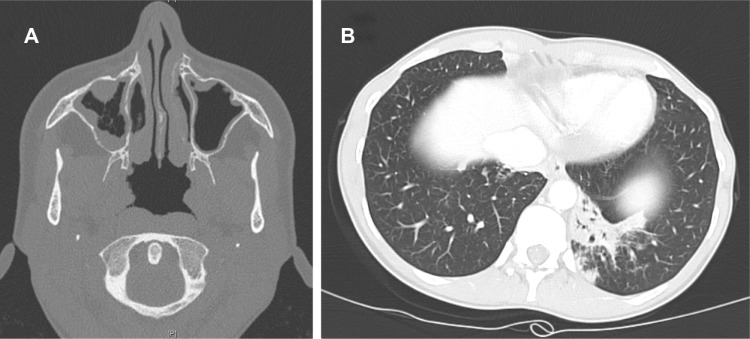
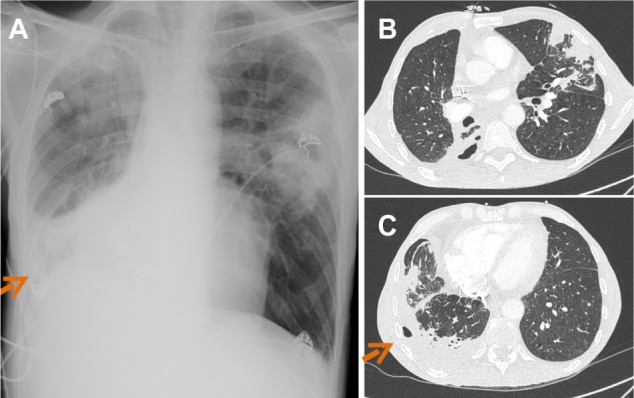
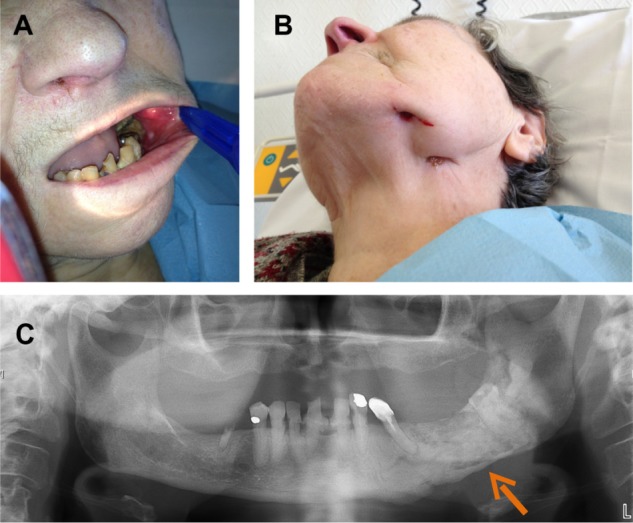
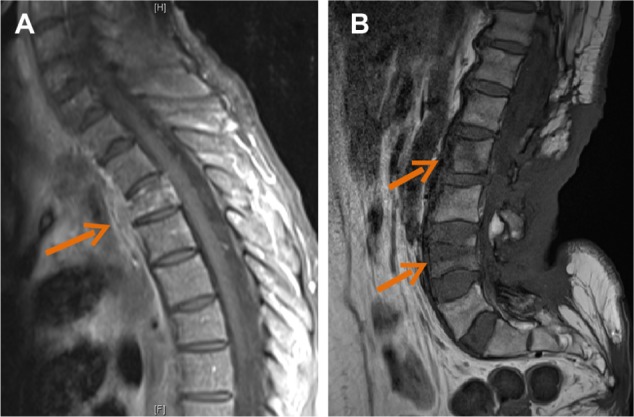
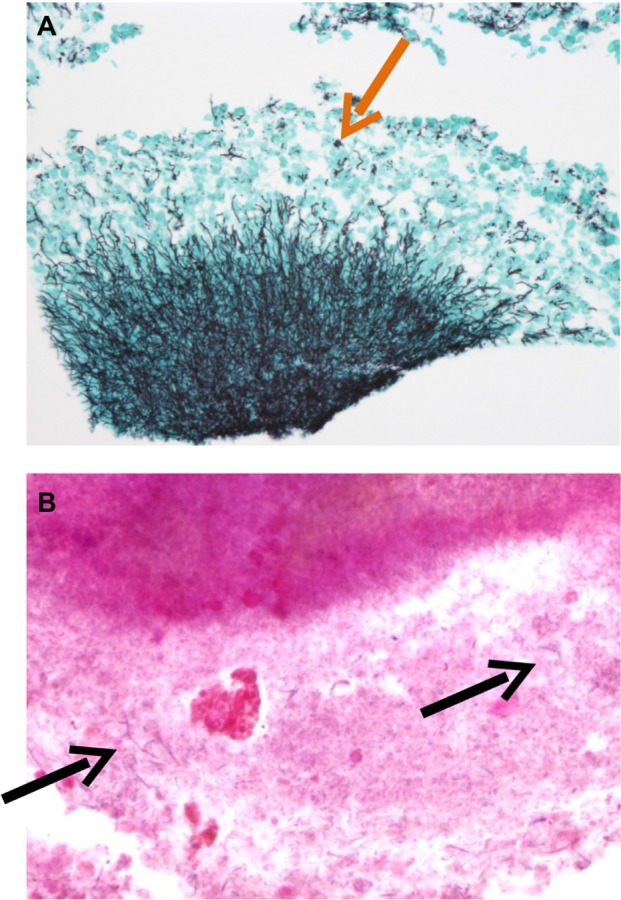
Actinomycosis is a rare chronic disease caused by Actinomyces spp., anaerobic Gram-positive bacteria that normally colonize the human mouth and digestive and genital tracts. Physicians must be aware of typical clinical presentations (such as cervicofacial actinomycosis following dental focus of infection, pelvic actinomycosis in women with an intrauterine device, and pulmonary actinomycosis in smokers with poor dental hygiene), but also that actinomycosis may mimic the malignancy process in various anatomical sites. Bacterial cultures and pathology are the cornerstone of diagnosis, but particular conditions are required in order to get the correct diagnosis. Prolonged bacterial cultures in anaerobic conditions are necessary to identify the bacterium and typical microscopic findings include necrosis with yellowish sulfur granules and filamentous Gram-positive fungal-like pathogens. Patients with actinomycosis require prolonged (6- to 12-month) high doses (to facilitate the drug penetration in abscess and in infected tissues) of penicillin G or amoxicillin, but the duration of antimicrobial therapy could probably be shortened to 3 months in patients in whom optimal surgical resection of infected tissues has been performed. Preventive measures, such as reduction of alcohol abuse and improvement of dental hygiene, may limit occurrence of pulmonary, cervicofacial, and central nervous system actinomycosis. In women, intrauterine devices must be changed every 5 years in order to limit the occurrence of pelvic actinomycosis.
Keywords: Actinomyces spp.; lumpy jaw syndrome; osteomyelitis; sulfur granule.
Figures



References
-
- Wong VK, Turmezei TD, Weston VC. Actinomycosis. BMJ. 2011;343:d6099. - PubMed
-
- Smego RA, Jr, Foglia G. Actinomycosis. Clin Infect Dis. 1998;26(6):1255–1261. - PubMed
-
- Mandell GL, Bennett JE, Dolin R, editors. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 7th ed. Philadelphia, PA: Churchill Livingstone Elsevier; 2010.
-
- Schaal KP, Lee HJ. Actinomycete infections in humans – a review. Gene. 1992;115(1–2):201–211. - PubMed
-
- Pulverer G, Schütt-Gerowitt H, Schaal KP. Human cervicofacial actinomycoses: microbiological data for 1997 cases. Clin Infect Dis. 2003;37(4):490–497. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
