

Radiofrequency ablation compared to surgery for the treatment of benign thyroid nodules
- PMID: 25045352
- PMCID: PMC4090443
- DOI: 10.1155/2014/934595
Radiofrequency ablation compared to surgery for the treatment of benign thyroid nodules
Abstract
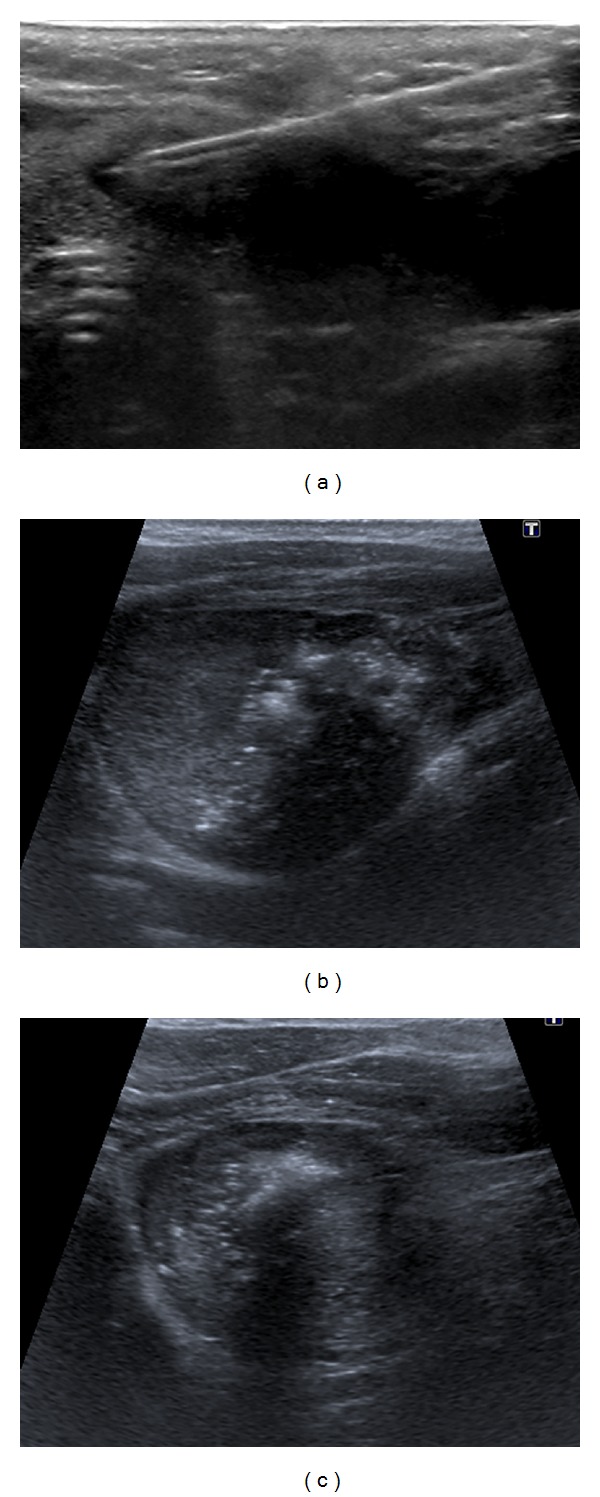
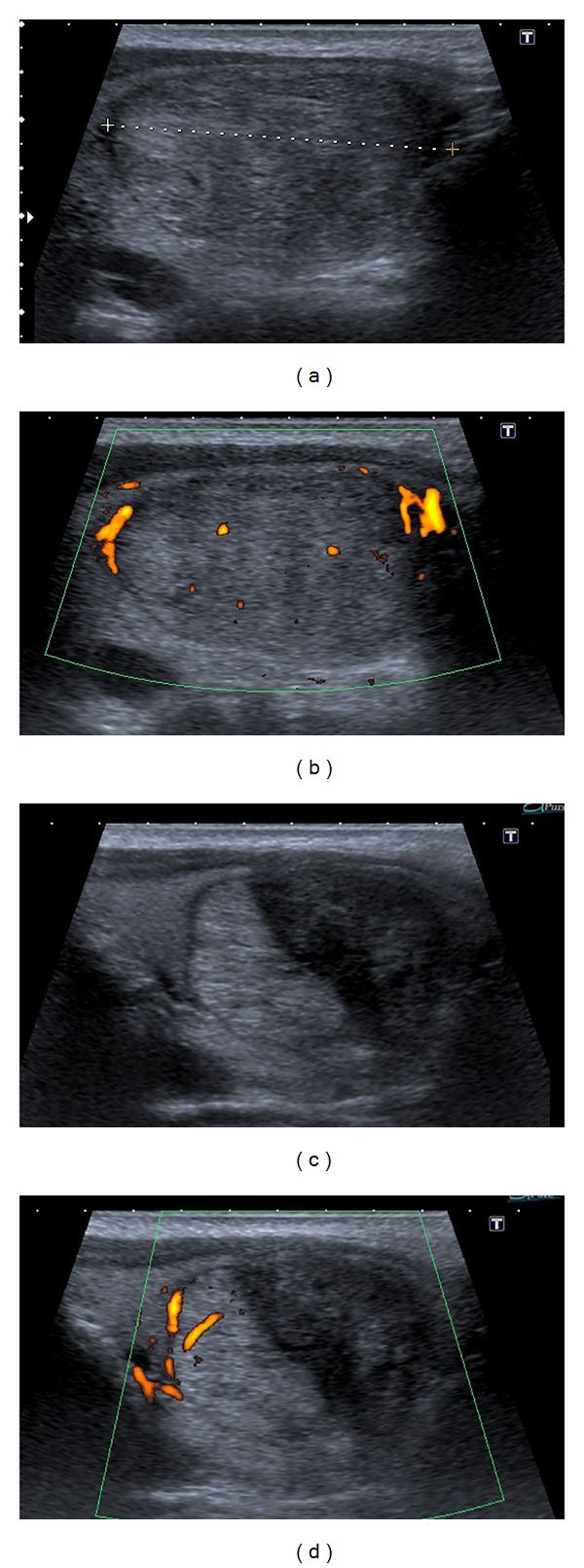
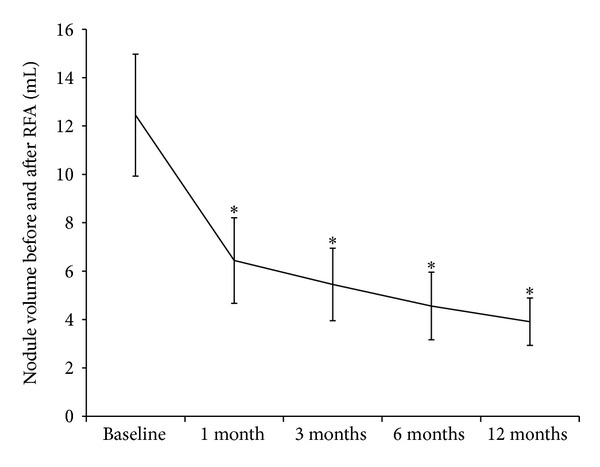
Objective. Benign thyroid nodules are a common occurrence whose only remedy, in case of symptoms, has always been surgery until the advent of new techniques, such as radiofrequency ablation (RFA). This study aimed at evaluating RFA efficacy, tolerability, and costs and comparing them to hemithyroidectomy for the treatment of benign thyroid nodules. Design and Methods. 37 patients who underwent RFA were retrospectively compared to 74 patients surgically treated, either in a standard inpatient or in a short-stay surgical regimen. Efficacy, tolerability, and costs were compared. The contribution of final pathology was also taken into account. Results. RFA reduced nodular volume by 70% after 12 months and it was an effective method for treating nodule-related clinical problems, but it was not as effective as surgery for the treatment of hot nodules. RFA and surgery were both safe, although RFA had less complications and pain was rare. RFA costed €1,661.50, surgery costed €4,556.30, and short-stay surgery costed €4,139.40 per patient. RFA, however, did not allow for any pathologic analysis of the nodules, which, in 6 patients who had undergone surgery (8%), revealed that the nodules harboured malignant cells. Conclusions. RFA might transform our approach to benign thyroid nodules.
Figures
References
-
- Mortensen JD, Woolner LB, Bennett WA. Gross and microscopic findings in clinically normal thyroid glands. The Journal of Clinical Endocrinology and Metabolism. 1955;15(10):1270–1280. - PubMed
-
- Tan GH, Gharib H. Thyroid incidentalomas: management approaches to nonpalpable nodules discovered incidentally on thyroid imaging. Annals of Internal Medicine. 1997;126(3):226–231. - PubMed
-
- Cooper DS, Doherty GM, Haugen BR, et al. Revised American thyroid association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19(11):1167–1214. - PubMed
-
- Gharib H, Papini E, Valcavi R, et al. American association of clinical endocrinologists and associazione medici endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. Endocrine Practice. 2006;12(1):63–102. - PubMed
-
- Reeve T, Thompson NW. Complications of thyroid surgery: how to avoid them, how to manage them, and observations on their possible effect on the whole patient. World Journal of Surgery. 2000;24(8):971–975. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
