

Risk factors for leptomeningeal carcinomatosis in patients with brain metastases who have previously undergone stereotactic radiosurgery
- PMID: 25048529
- PMCID: PMC10329461
- DOI: 10.1007/s11060-014-1539-6
Risk factors for leptomeningeal carcinomatosis in patients with brain metastases who have previously undergone stereotactic radiosurgery
Abstract
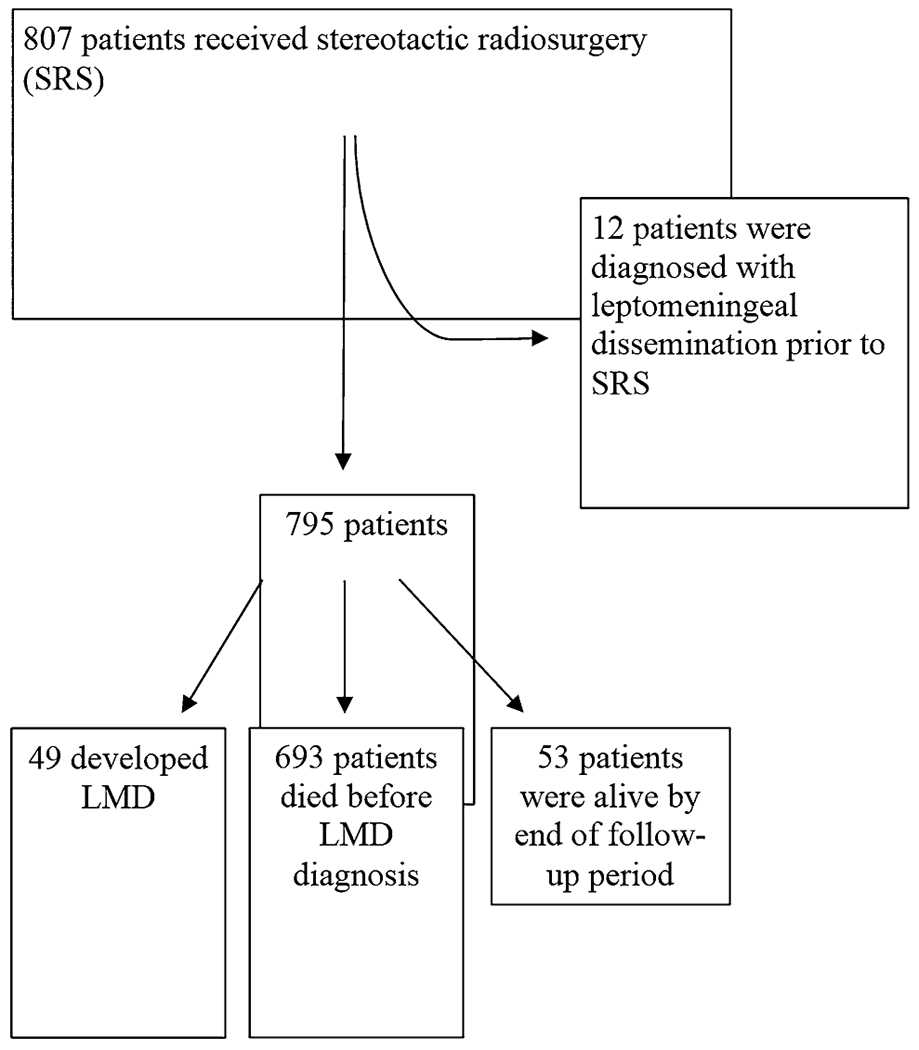
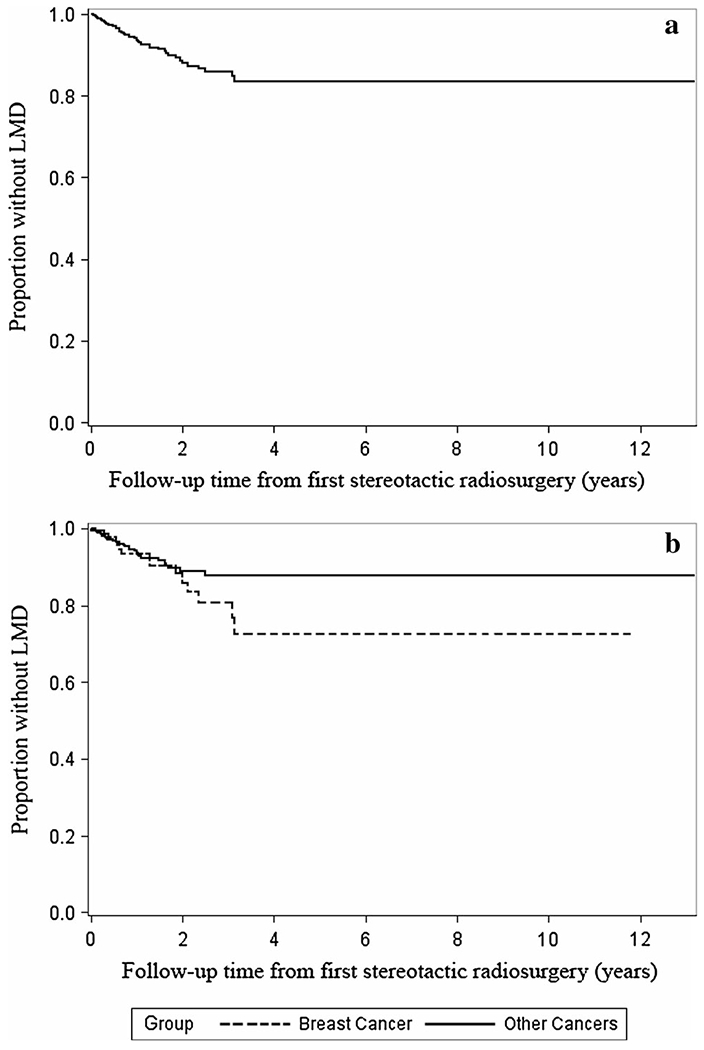
Our objective was to explore the hypothesis that the risk of leptomeningeal dissemination (LMD) in patients who underwent stereotactic radiosurgery (SRS) for brain metastases is influenced by the site of the primary cancer, the addition of whole brain radiation therapy (WBRT), surgical resection, and control over their systemic disease. We conducted a retrospective cohort analysis of 805 patients who were treated with SRS for brain metastases between 1999 and 2012 at the Wake Forest Baptist Medical Center, and excluded all patients with evidence of LMD before SRS. The primary outcome was LMD. Forty-nine of 795 patients developed LMD with a cumulative incidence of 6.2% (95% Confidence Interval (CI), 4.7-8.0). Median time from SRS to LMD was 7.4 months (Interquartile Range (IQR), 3.3-15.4). A colorectal primary site (Hazard Ratio (HR), 4.5; 95% CI 2.5-8.0; p < 0.0001), distant brain failure (HR, 2.0; 95% CI 1.2-3.2; p = 0.007), breast primary site (HR, 1.6; 95% CI 1.0-2.7; p = 0.05), the number of intracranial metastases at time of initial SRS (HR, 1.1; 95% CI 1.0-1.2; p = 0.02), and age (by 5-year interval) (HR, 0.9; 95% CI 0.8, 0.9; p = 0.0006) were independent factors associated with LMD. There was no evidence that surgical resection before SRS altered the risk of LMD (HR, 1.1; 95 % CI 0.6-2.0, p = 0.78). In patients who underwent SRS for brain metastases, a colorectal or breast primary site, distant brain failure, younger age, and an increased number of intracranial metastases were independently associated with LMD. Given its relative rarity as an outcome, multi-institutional prospective studies will likely be necessary to validate and quantify these relationships.
Figures
References
-
- Loganathan AG, Chan MD, Alphonse N et al. (2012) Clinical outcomes of brain metastases treated with Gamma Knife radiosurgery with 3.0 T versus 1.5 T MRI-based treatment planning: have we finally optimised detection of occult brain metastases? J Med Imaging Radiat Oncol 56:554–560 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
