

Association of non-alcoholic fatty liver disease with chronic kidney disease: a systematic review and meta-analysis
- PMID: 25050550
- PMCID: PMC4106719
- DOI: 10.1371/journal.pmed.1001680
Association of non-alcoholic fatty liver disease with chronic kidney disease: a systematic review and meta-analysis
Abstract
Background: Chronic kidney disease (CKD) is a frequent, under-recognized condition and a risk factor for renal failure and cardiovascular disease. Increasing evidence connects non-alcoholic fatty liver disease (NAFLD) to CKD. We conducted a meta-analysis to determine whether the presence and severity of NAFLD are associated with the presence and severity of CKD.
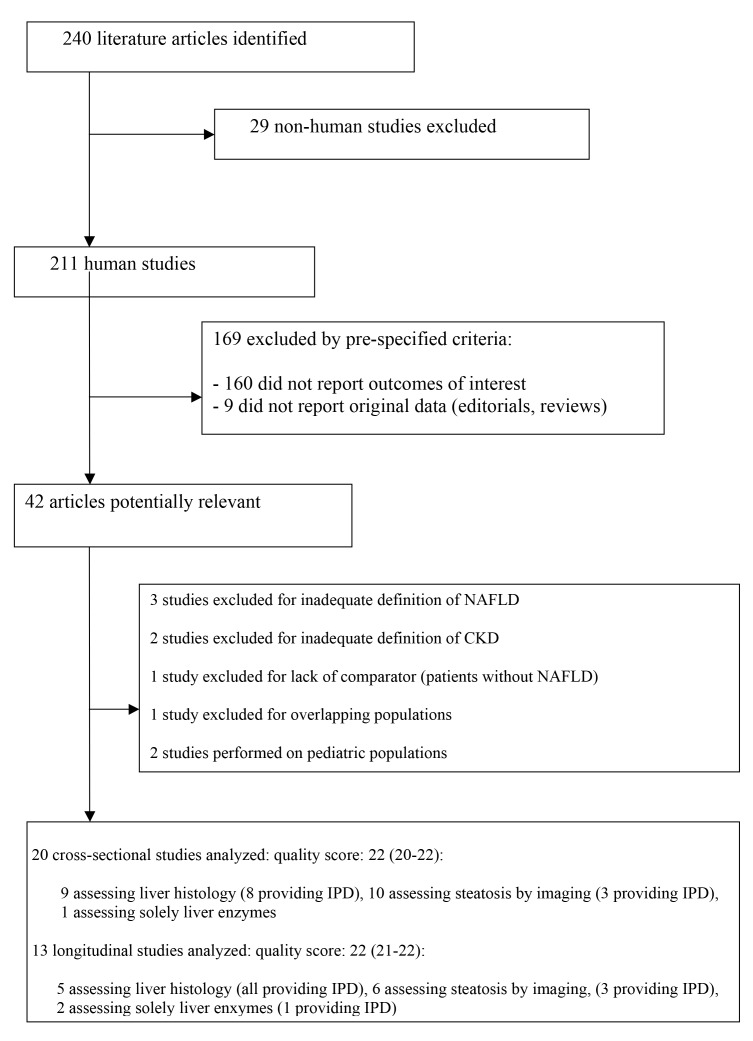
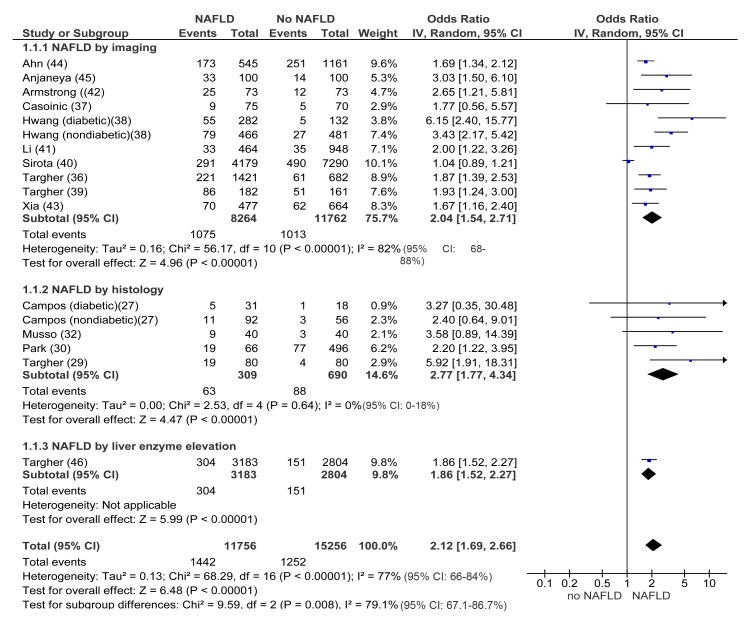
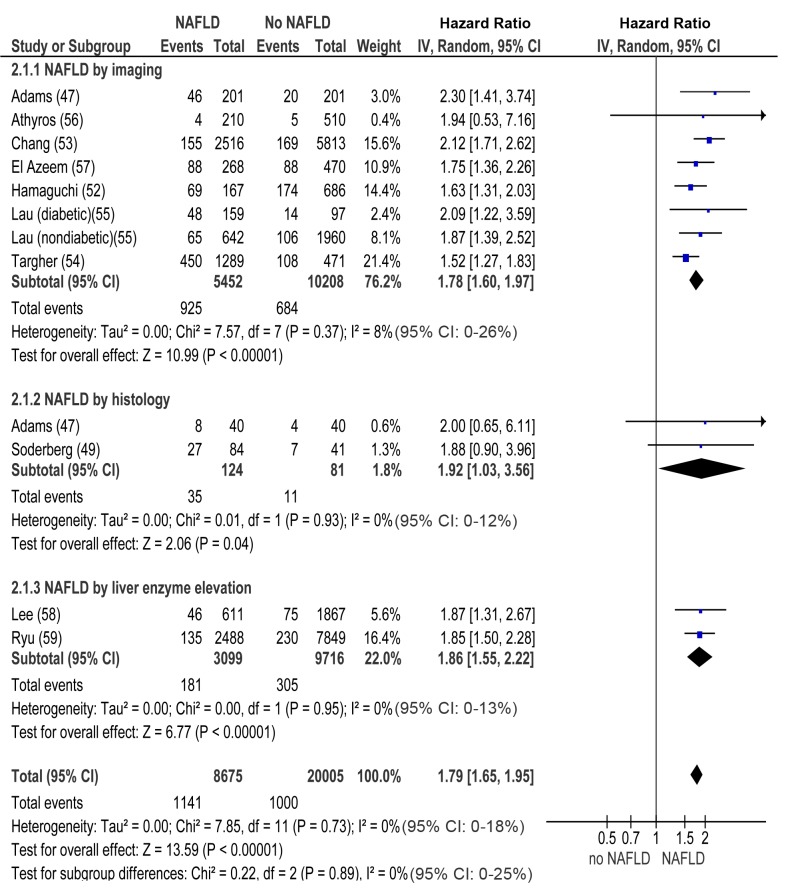
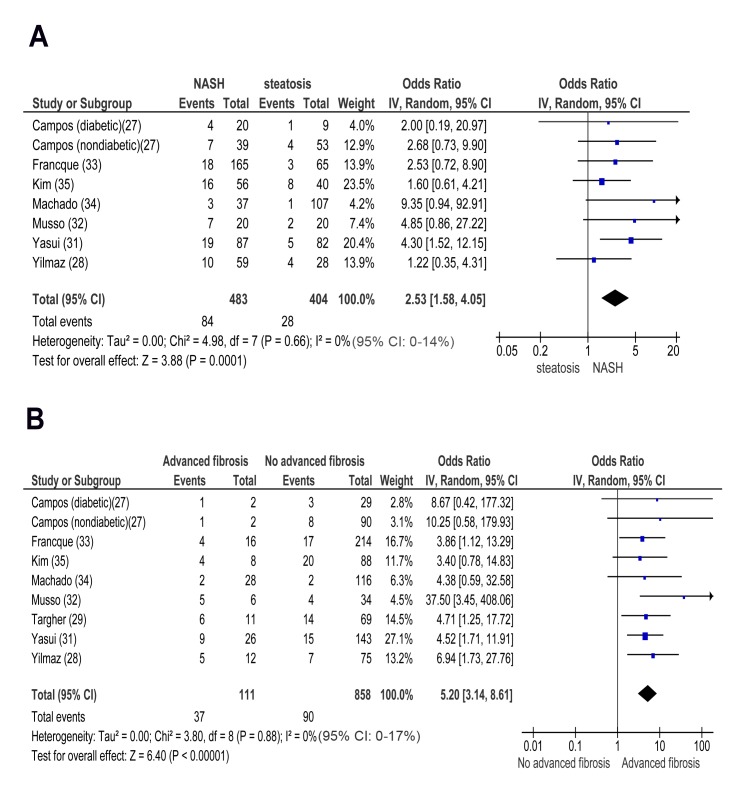
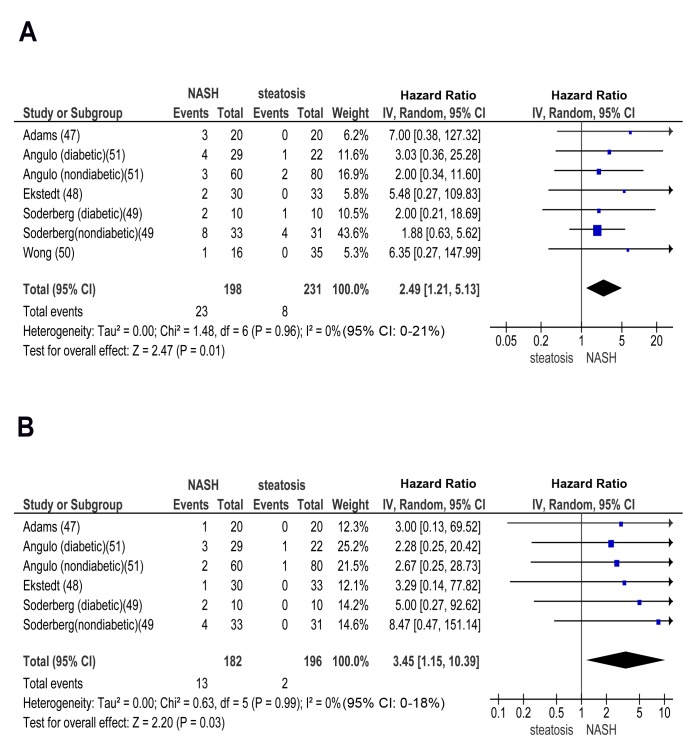
Methods and findings: English and non-English articles from international online databases from 1980 through January 31, 2014 were searched. Observational studies assessing NAFLD by histology, imaging, or biochemistry and defining CKD as either estimated glomerular filtration rate (eGFR) <60 ml/min/1.73 m2 or proteinuria were included. Two reviewers extracted studies independently and in duplicate. Individual participant data (IPD) were solicited from all selected studies. Studies providing IPD were combined with studies providing only aggregate data with the two-stage method. Main outcomes were pooled using random-effects models. Sensitivity and subgroup analyses were used to explore sources of heterogeneity and the effect of potential confounders. The influences of age, whole-body/abdominal obesity, homeostasis model of insulin resistance (HOMA-IR), and duration of follow-up on effect estimates were assessed by meta-regression. Thirty-three studies (63,902 participants, 16 population-based and 17 hospital-based, 20 cross-sectional, and 13 longitudinal) were included. For 20 studies (61% of included studies, 11 cross-sectional and nine longitudinal, 29,282 participants), we obtained IPD. NAFLD was associated with an increased risk of prevalent (odds ratio [OR] 2.12, 95% CI 1.69-2.66) and incident (hazard ratio [HR] 1.79, 95% CI 1.65-1.95) CKD. Non-alcoholic steatohepatitis (NASH) was associated with a higher prevalence (OR 2.53, 95% CI 1.58-4.05) and incidence (HR 2.12, 95% CI 1.42-3.17) of CKD than simple steatosis. Advanced fibrosis was associated with a higher prevalence (OR 5.20, 95% CI 3.14-8.61) and incidence (HR 3.29, 95% CI 2.30-4.71) of CKD than non-advanced fibrosis. In all analyses, the magnitude and direction of effects remained unaffected by diabetes status, after adjustment for other risk factors, and in other subgroup and meta-regression analyses. In cross-sectional and longitudinal studies, the severity of NAFLD was positively associated with CKD stages. Limitations of analysis are the relatively small size of studies utilizing liver histology and the suboptimal sensitivity of ultrasound and biochemistry for NAFLD detection in population-based studies.
Conclusion: The presence and severity of NAFLD are associated with an increased risk and severity of CKD. Please see later in the article for the Editors' Summary.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



Comment in
-
Does diagnosing fatty liver and chronic kidney disease do more good than harm?PLoS Med. 2014 Jul 22;11(7):e1001681. doi: 10.1371/journal.pmed.1001681. eCollection 2014 Jul. PLoS Med. 2014. PMID: 25050619 Free PMC article.
References
-
- McCullough K, Sharma P, Ali T, Khan I, Smith WC, et al. (2012) Measuring the population burden of chronic kidney disease: a systematic literature review of the estimated prevalence of impaired kidney function. Nephrol Dial Transplant 27: 1812–1821. - PubMed
-
- Stevens PE, Levin A (2013) A Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members (2013) Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med 158: 825–830. - PubMed
-
- James MT, Hemmelgarn BR, Tonelli M (2010) Early recognition and prevention of chronic kidney disease. Lancet 375: 1296–1309. - PubMed
-
- Herzog CA, Asinger RW, Berger AK, Charytan DM, Dıez J, et al. (2011) Cardiovascular disease in chronic kidney disease. A clinical update from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int 80: 572–586. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
