

MRI of axillary brachial plexus blocks: a randomised controlled study
- PMID: 25051144
- PMCID: PMC4196799
- DOI: 10.1097/EJA.0000000000000122
MRI of axillary brachial plexus blocks: a randomised controlled study
Abstract
Background: Axillary plexus blocks are usually guided by ultrasound, but alternative methods may be used when ultrasound equipment is lacking. For a nonultrasound-guided axillary block, the need for three injections has been questioned.
Objectives: Could differences in block success between single, double and triple deposits methods be explained by differences in local anaesthetic distribution as observed by MRI?
Design: A blinded and randomised controlled study.
Setting: Conducted at Oslo University Hospital, Rikshospitalet, Norway from 2009 to 2011.
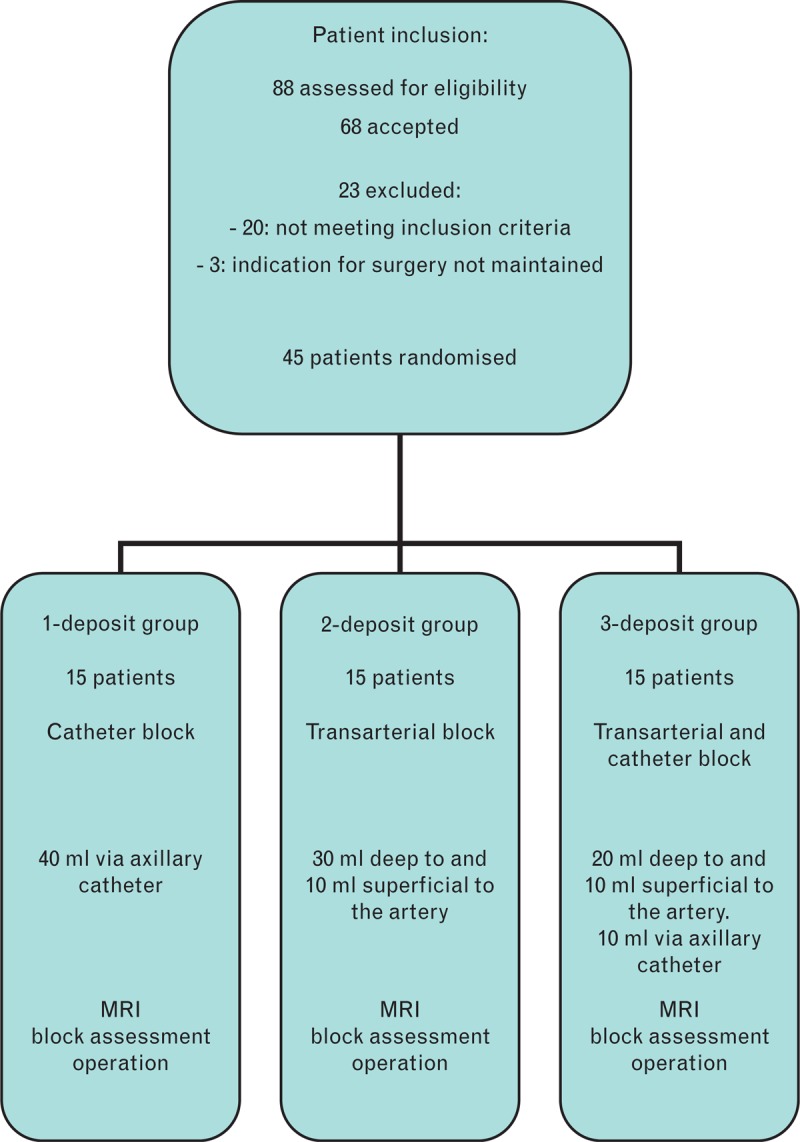
Patients: Forty-five ASA 1 to 2 patients scheduled for surgery were randomised to three equally sized groups. All patients completed the study.
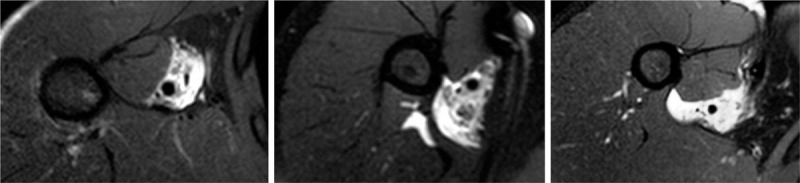
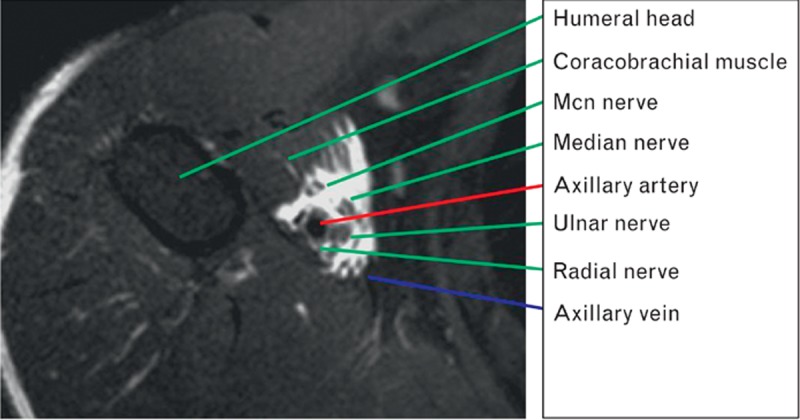
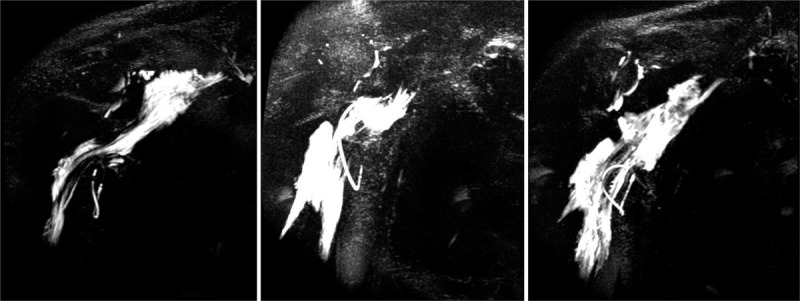
Interventions: Patients in the single-deposit group had an injection through a catheter parallel to the median nerve. In the double-deposit group the patients received a transarterial block. In the triple-deposit group the injections of the two other groups were combined. Upon completion of local anaesthetic injection the patients were scanned by MRI, before clinical block assessment. The distribution of local anaesthetic was scored by its closeness to terminal nerves and cords of the brachial plexus, as seen by MRI. The clinical effect was scored by the degree of sensory block in terminal nerve innervation areas.
Main outcome measures: Sensory block effect and MRI distribution pattern.
Results: The triple-deposit method had a higher success rate (100%) than the single-deposit method (67%) and the double-deposit method (67%) in blocking all cutaneous nerves distal to the elbow (P = 0.04). The patients in the triple-deposit group most often had the best MRI scores. For any nerve or cord, at least one of the single-deposit or double-deposit groups had a similarly high MRI score as the triple-deposit group.
Conclusion: Distal to the elbow, the triple-deposit method had the highest sensory block success rate. This could be explained to some extent by analysis of the magnetic resonance images.
Trial registration: ClinicalTrials.gov identifier: NCT01033006.
Figures
Similar articles
-
Double-injection technique assisted by a nerve stimulator for ultrasound-guided supraclavicular brachial plexus block results in better distal sensory-motor block: A randomised controlled trial.Eur J Anaesthesiol. 2017 Mar;34(3):127-134. doi: 10.1097/EJA.0000000000000542. Eur J Anaesthesiol. 2017. PMID: 27798452 Clinical Trial.
-
Efficacy of axillary versus infraclavicular brachial plexus block in preventing tourniquet pain: A randomised trial.Eur J Anaesthesiol. 2019 Jan;36(1):48-54. doi: 10.1097/EJA.0000000000000928. Eur J Anaesthesiol. 2019. PMID: 30461447 Clinical Trial.
-
Retroclavicular vs supraclavicular brachial plexus block for distal upper limb surgery: a randomised, controlled, single-blinded trial.Br J Anaesth. 2019 Apr;122(4):518-524. doi: 10.1016/j.bja.2018.12.022. Epub 2019 Jan 31. Br J Anaesth. 2019. PMID: 30857608 Free PMC article. Clinical Trial.
-
Comparison of ultrasound and ultrasound plus nerve stimulator guidance axillary plexus block.J Pak Med Assoc. 2017 Apr;67(4):508-512. J Pak Med Assoc. 2017. PMID: 28420906 Clinical Trial.
-
The ultrasound-guided selective nerve block in the upper arm: an approach of retaining the motor function in elbow.BMC Anesthesiol. 2018 Oct 19;18(1):143. doi: 10.1186/s12871-018-0584-7. BMC Anesthesiol. 2018. PMID: 30340524 Free PMC article. Clinical Trial.
Cited by
-
Single, double or multiple-injection techniques for non-ultrasound guided axillary brachial plexus block in adults undergoing surgery of the lower arm.Cochrane Database Syst Rev. 2016 Sep 2;9(9):CD003842. doi: 10.1002/14651858.CD003842.pub5. Cochrane Database Syst Rev. 2016. PMID: 27589694 Free PMC article. Review.
-
The relationship of the musculocutaneous nerve to the brachial plexus evaluated by MRI.J Clin Monit Comput. 2017 Feb;31(1):111-115. doi: 10.1007/s10877-015-9807-3. Epub 2015 Nov 19. J Clin Monit Comput. 2017. PMID: 26584952 Free PMC article.
-
A randomised, non-inferiority study of chloroprocaine 2% and ropivacaine 0.75% in ultrasound-guided axillary block.Sci Rep. 2021 May 11;11(1):10035. doi: 10.1038/s41598-021-89483-y. Sci Rep. 2021. PMID: 33976374 Free PMC article. Clinical Trial.
References
-
- Thompson GE, Rorie DK. Functional anatomy of the brachial plexus sheaths. Anesthesiology 1983; 59:117–122 - PubMed
-
- Koscielniak-Nielsen ZJ, Stens-Pedersen HL, Lippert FK. Readiness for surgery after axillary block: single or multiple injection techniques. Eur J Anaesthesiol 1997; 14:164–171 - PubMed
-
- Chan VW, Perlas A, McCartney CJ, et al. Ultrasound guidance improves success rate of axillary brachial plexus block. Can J Anaesth 2007; 54:176–182 - PubMed
-
- Kjelstrup T. Transarterial block as an addition to a conventional catheter technique improves the axillary block. Acta Anaesthesiol Scand 2006; 50:112–116 - PubMed
-
- Landsverk SA, Kvandal P, Kjelstrup T, et al. Human skin microcirculation after brachial plexus block evaluated by wavelet transform of the laser Doppler flowmetry signal. Anesthesiology 2006; 105:478–484 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
