

Quantitative measurement of elasticity of the appendix using shear wave elastography in patients with suspected acute appendicitis
- PMID: 25051242
- PMCID: PMC4106760
- DOI: 10.1371/journal.pone.0101292
Quantitative measurement of elasticity of the appendix using shear wave elastography in patients with suspected acute appendicitis
Abstract
Introduction: Shear wave elastography (SWE) has not been studied for diagnosing appendicitis. We postulated that an inflamed appendix would become stiffer than a normal appendix. We evaluated the elastic modulus values (EMV) by SWE in healthy volunteers, patients without appendicitis, and patients with appendicitis. We also evaluated diagnostic ability of SWE for differentiating an inflamed from a normal appendix in patients with suspected appendicitis.
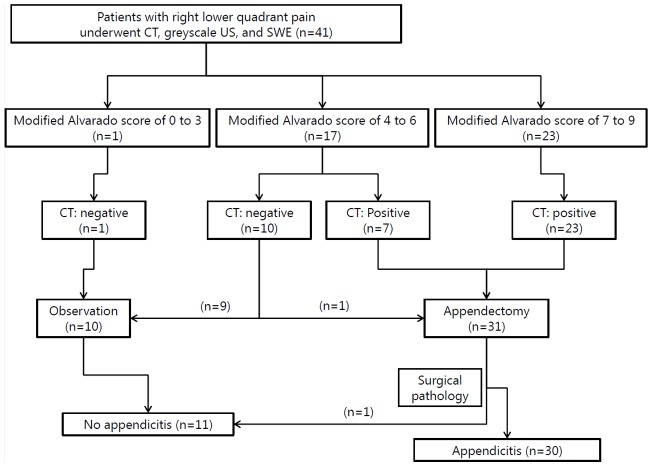
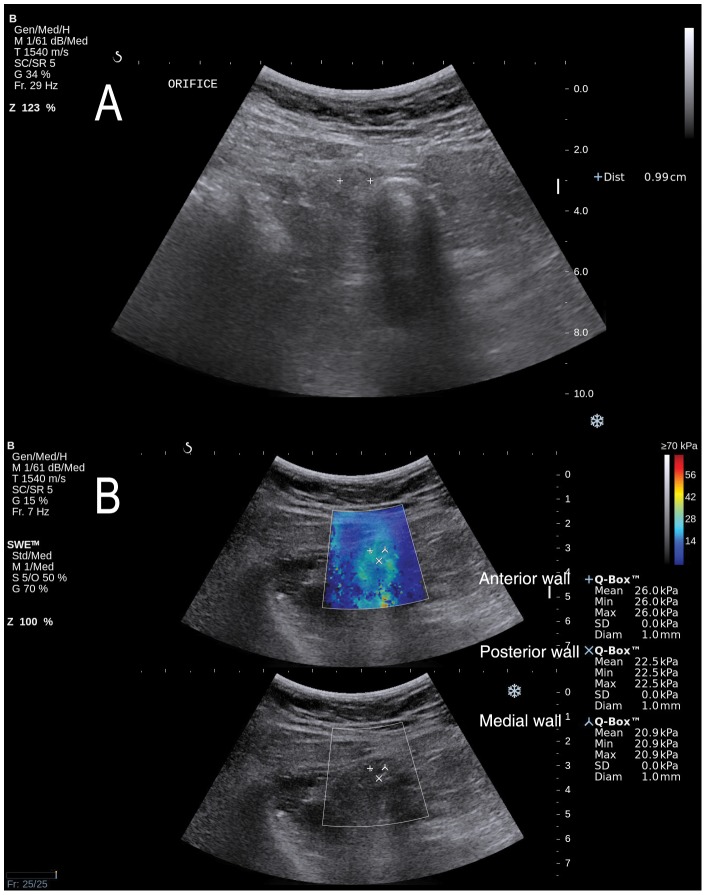
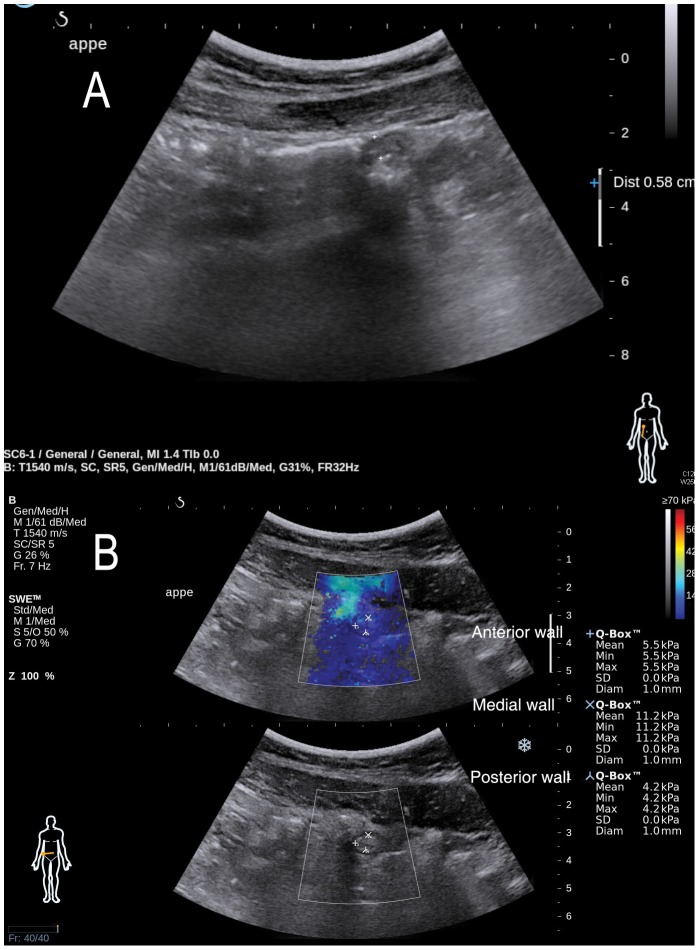
Materials and methods: Forty-one patients with clinically suspected acute appendicitis and 11 healthy volunteers were prospectively enrolled. Gray-scale ultrasonography (US), SWE and multi-slice computed tomography (CT) were performed. The EMV was measured in the anterior, medial, and posterior appendiceal wall using SWE, and the highest value (kPa) was recorded.
Results: Patients were classified into appendicitis (n = 30) and no appendicitis groups (n = 11). One case of a negative appendectomy was detected. The median EMV was significantly higher in the appendicitis group (25.0 kPa) compared to that in the no appendicitis group (10.4 kPa) or in the healthy controls (8.3 kPa) (p<0.001). Among SWE and other US and CT features, CT was superior to any conventional gray-scale US feature or SWE. Either the CT diameter criterion or combined three CT features predicted true positive in 30 and true negative in 11 cases and yielded 100% sensitivity and 100% specificity. An EMV of 12.5 kPa for the stiffest region of the appendix predicted true positive in 28, true negative in 11, and false negative in two cases. The EMV (≥12.5 kPa) yielded 93% sensitivity and 100% specificity.
Conclusion: Our results suggest that EMV by SWE helps distinguish an inflamed from a normal appendix. Given that SWE has high specificity, quantitative measurement of the elasticity of the appendix may provide complementary information, in addition to morphologic features on gray-scale US, in the diagnosis of appendicitis.
Conflict of interest statement
Figures
References
-
- Balthazar EJ, Rofsky NM, Zucker R (1998) Appendicitis: the impact of computed tomography imaging on negative appendectomy and perforation rates. Am J Gastroenterol 93: 768–771. - PubMed
-
- Brandt MM, Wahl WL (2003) Liberal use of CT scanning helps to diagnose appendicitis in adults. Am Surg 69: 727–731 discussion 731–722. - PubMed
-
- Rettenbacher T, Hollerweger A, Macheiner P, Rettenbacher L, Frass R, et al. (2000) Presence or absence of gas in the appendix: additional criteria to rule out or confirm acute appendicitis–evaluation with US. Radiology 214: 183–187. - PubMed
-
- van Randen A, Bipat S, Zwinderman AH, Ubbink DT, Stoker J, et al. (2008) Acute appendicitis: meta-analysis of diagnostic performance of CT and graded compression US related to prevalence of disease. Radiology 249: 97–106. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
